También podría gustarte
- Article SCL 10Documento21 páginasArticle SCL 10Erlina RatmayantiAún no hay calificaciones
- The Psychometric Property of The Short Thai Version of The Philadelphia Mindfulness ScaleDocumento7 páginasThe Psychometric Property of The Short Thai Version of The Philadelphia Mindfulness ScaleCocaAún no hay calificaciones
- 2011 - IJCHP - The Leyton Obsessional Inventory-Child VersionDocumento16 páginas2011 - IJCHP - The Leyton Obsessional Inventory-Child VersionEsteysi Villarroel BernalesAún no hay calificaciones
- IPO-artikel MenningerBulletin 2009Documento17 páginasIPO-artikel MenningerBulletin 2009Feras ZidiAún no hay calificaciones
- D S 90 (SCL 90) : Ymptom Heck ISTDocumento10 páginasD S 90 (SCL 90) : Ymptom Heck ISTMax ImoAún no hay calificaciones
- Caraveo 2007Documento8 páginasCaraveo 2007Karla SuárezAún no hay calificaciones
- Rating Scales Validated For Sri Lankan PopulationsDocumento9 páginasRating Scales Validated For Sri Lankan PopulationsMatt AldridgeAún no hay calificaciones
- Practice Reading 1 - PassageDocumento8 páginasPractice Reading 1 - PassageValiant CheungAún no hay calificaciones
- Psychometric Properties of Lock-Wallace Short Marital Adjustment Scale (Lwsmas) For Bangladeshi CouplesDocumento7 páginasPsychometric Properties of Lock-Wallace Short Marital Adjustment Scale (Lwsmas) For Bangladeshi CouplesSrishti GaurAún no hay calificaciones
- Cognitive Emotion Regulation Questionnaire - Development of A Short 18-Item Version (CERQ-short)Documento9 páginasCognitive Emotion Regulation Questionnaire - Development of A Short 18-Item Version (CERQ-short)leonardAún no hay calificaciones
- Accesare - Resursa 3Documento31 páginasAccesare - Resursa 3Rodica Pentea-PopAún no hay calificaciones
- The Menopause Rating Scale (MRS)Documento8 páginasThe Menopause Rating Scale (MRS)Nurfadila RasyidAún no hay calificaciones
- Rating Scales Validated For Sri Lankan PopulationsDocumento9 páginasRating Scales Validated For Sri Lankan PopulationsDilukshi WickramasingheAún no hay calificaciones
- Ghassemzadeh Et Al, 2006Documento11 páginasGhassemzadeh Et Al, 2006Aref TabahoriAún no hay calificaciones
- The Psychopathy ChecklistDocumento21 páginasThe Psychopathy ChecklistAhmad Fauzi100% (3)
- Reliability and Factor Structure of The Chinese Version of Childhood Trauma Questionnaire-Short Form in in Patients With Substance Use DisorderDocumento11 páginasReliability and Factor Structure of The Chinese Version of Childhood Trauma Questionnaire-Short Form in in Patients With Substance Use Disorderafro stAún no hay calificaciones
- Factor Structure of SA-45 Questionnaire in Non-Clinical Spanish SampleDocumento12 páginasFactor Structure of SA-45 Questionnaire in Non-Clinical Spanish SampleGonzalo Morán MoránAún no hay calificaciones
- The Role of IL-6 For Predicting Neonatal Sepsis: A Systematic Review and Meta-AnalysisDocumento7 páginasThe Role of IL-6 For Predicting Neonatal Sepsis: A Systematic Review and Meta-AnalysisFrancisco Chávez SolsolAún no hay calificaciones
- Schizophr Bull 1987 Kay 261 76Documento16 páginasSchizophr Bull 1987 Kay 261 76lucicosoAún no hay calificaciones
- The Development and Validation of The Philippine National Police Wellbeing Scale (Pnp-Wells)Documento13 páginasThe Development and Validation of The Philippine National Police Wellbeing Scale (Pnp-Wells)Joven Gerald ObanilAún no hay calificaciones
- Obsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsDocumento6 páginasObsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsJorge VelardeAún no hay calificaciones
- Boulet & Boss, 1991Documento5 páginasBoulet & Boss, 1991mazfarsAún no hay calificaciones
- Assignment in Psychological AssessmentDocumento16 páginasAssignment in Psychological Assessmentale.cristianAún no hay calificaciones
- Validation of An Emotional Intelligence Scale - A Case of An AfricDocumento8 páginasValidation of An Emotional Intelligence Scale - A Case of An Africhabeeb UppinangadyAún no hay calificaciones
- Escala Ansietat Parkinson (PAS)Documento55 páginasEscala Ansietat Parkinson (PAS)Mar BatistaAún no hay calificaciones
- The Use of The Personality Assessment Inventory (PAI) in Assessing OffendersDocumento17 páginasThe Use of The Personality Assessment Inventory (PAI) in Assessing OffendersgenerjustnAún no hay calificaciones
- The Maudsley Obsessive-Compulsive Inventory: A Reliability Generalization Meta-AnalysisDocumento21 páginasThe Maudsley Obsessive-Compulsive Inventory: A Reliability Generalization Meta-AnalysisGiorgioD.KotzalidisAún no hay calificaciones
- Translation and Validation of Symptom Checklist-90: Nadia Shafique and Muhammad Tahir KhalilyDocumento17 páginasTranslation and Validation of Symptom Checklist-90: Nadia Shafique and Muhammad Tahir Khalilyaneela khanAún no hay calificaciones
- Validity of Autism Behavior Checklist (ABC)Documento7 páginasValidity of Autism Behavior Checklist (ABC)Victória NamurAún no hay calificaciones
- Teste Faux PasDocumento5 páginasTeste Faux PasAdriano FerrazAún no hay calificaciones
- RCADS Clinical (Chorpita, Moffitt, Gray)Documento14 páginasRCADS Clinical (Chorpita, Moffitt, Gray)Paula MacielAún no hay calificaciones
- CuestionarioEscolaresyAdolLtTAHValidezsaludmental20093263 68Documento6 páginasCuestionarioEscolaresyAdolLtTAHValidezsaludmental20093263 68Madeline MirandaAún no hay calificaciones
- Anxiety EpidemiologyDocumento14 páginasAnxiety EpidemiologyelvineAún no hay calificaciones
- This DescriptiveDocumento1 páginaThis DescriptiveAinaazharAún no hay calificaciones
- 10 1007BF00805437Documento5 páginas10 1007BF00805437Vũ Nguyễn Cao HuyAún no hay calificaciones
- PsNP07-08.04 Blazevska - Stoilkovska, B., Naumova, KDocumento15 páginasPsNP07-08.04 Blazevska - Stoilkovska, B., Naumova, KBorjan AdziskiAún no hay calificaciones
- Assessing sensory processing in children and adolescents with autismDocumento27 páginasAssessing sensory processing in children and adolescents with autismvyzze kAún no hay calificaciones
- Validity of The DSM-Oriented Scales of The Child Behavior Checklist and Youth Self-ReportDocumento8 páginasValidity of The DSM-Oriented Scales of The Child Behavior Checklist and Youth Self-ReportJojanna P. Parada MedinaAún no hay calificaciones
- PHQ-9 PresentationDocumento35 páginasPHQ-9 PresentationWYNONA LIMAún no hay calificaciones
- Purchase Tests For Clinical UseDocumento9 páginasPurchase Tests For Clinical UseCristy PagalanAún no hay calificaciones
- The Fivefactor Structure of The Panss A Critical Review of Its Consistency Across StudiesDocumento8 páginasThe Fivefactor Structure of The Panss A Critical Review of Its Consistency Across StudiesHosam AAAún no hay calificaciones
- Fulltext - Depression v5 Id1097Documento4 páginasFulltext - Depression v5 Id1097Oscar EsparzaAún no hay calificaciones
- Is Disorganized Schizophrenia A Predictor of Treatment Resistance? Evidence From An Observational StudyDocumento3 páginasIs Disorganized Schizophrenia A Predictor of Treatment Resistance? Evidence From An Observational StudyTri WidiantoAún no hay calificaciones
- Blanchard Et Al 1996 Psychometric Properties of The PTSD Checklist (PCL)Documento5 páginasBlanchard Et Al 1996 Psychometric Properties of The PTSD Checklist (PCL)Florina AnichitoaeAún no hay calificaciones
- Psychometric Properties of The Chinese Version of The Psycho-Educational Profile-Revised (CPEP-R)Documento9 páginasPsychometric Properties of The Chinese Version of The Psycho-Educational Profile-Revised (CPEP-R)Charmaine Tuanqui MariscotesAún no hay calificaciones
- Grot 202000723Documento18 páginasGrot 202000723Nurdiana Julianti NoorAún no hay calificaciones
- Relationship between emotional intelligence and quality of life in cancer patientsDocumento6 páginasRelationship between emotional intelligence and quality of life in cancer patientsletter2lalAún no hay calificaciones
- Predicting PTSD From The Child Behavior Checklist - Data From A Field Study With Children and Adolescents in Foster CareDocumento6 páginasPredicting PTSD From The Child Behavior Checklist - Data From A Field Study With Children and Adolescents in Foster CareDonald Cabrera AstudilloAún no hay calificaciones
- Test Performance and Classification Statistics For The Rey Auditory Verbal Learning Test in Selected Clinical SamplesDocumento11 páginasTest Performance and Classification Statistics For The Rey Auditory Verbal Learning Test in Selected Clinical SamplesPatriciaAún no hay calificaciones
- Characteristics of Aphasia Research ParticipantsDocumento12 páginasCharacteristics of Aphasia Research ParticipantsLean ParkAún no hay calificaciones
- Relationship Between Premorbid Functioning and Symptom Severity As Assessed at First Episode of PsychosisDocumento6 páginasRelationship Between Premorbid Functioning and Symptom Severity As Assessed at First Episode of Psychosisaldrin19Aún no hay calificaciones
- NEO PI SummaryDocumento12 páginasNEO PI SummaryRoseNTolentinoAún no hay calificaciones
- Borderline Personality DisorderDocumento6 páginasBorderline Personality DisorderPersephona13Aún no hay calificaciones
- Telephone Validation of The Quality of Life in Epilepsy Inventory 89 (QOLIE 89)Documento10 páginasTelephone Validation of The Quality of Life in Epilepsy Inventory 89 (QOLIE 89)David DeegbeAún no hay calificaciones
- 7 MahamadulDocumento9 páginas7 MahamadulMMhasan SagarAún no hay calificaciones
- Sentence Completion TestsDocumento14 páginasSentence Completion TestsDoina Albescu60% (5)
- A Parent-Report Measure of Children's Anxiety Psychometric Properties and Comparison With Child-Report in A Clinic and Normal SampleDocumento27 páginasA Parent-Report Measure of Children's Anxiety Psychometric Properties and Comparison With Child-Report in A Clinic and Normal SampleAndreea CiobanAún no hay calificaciones
- The Little Black Book of Neuropsychology: A Syndrome-Based ApproachDe EverandThe Little Black Book of Neuropsychology: A Syndrome-Based ApproachCalificación: 5 de 5 estrellas5/5 (2)
- Dimensional PsychopathologyDe EverandDimensional PsychopathologyMassimo BiondiAún no hay calificaciones
- Developmental Follow-Up: Concepts, Domains, and MethodsDe EverandDevelopmental Follow-Up: Concepts, Domains, and MethodsAún no hay calificaciones
- Ba - Bacterial Identification Lab WorksheetDocumento12 páginasBa - Bacterial Identification Lab WorksheetFay SAún no hay calificaciones
- BenzophenoneDocumento20 páginasBenzophenoneYuuki93Aún no hay calificaciones
- LabTec Product SpecificationsDocumento292 páginasLabTec Product SpecificationsDiego TobrAún no hay calificaciones
- Prevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDDocumento7 páginasPrevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDMusainah FeisalAún no hay calificaciones
- GIGITAN ULAR BERBISA: GEJALA, PENANGANAN DAN JENIS ULAR PALING BERBISADocumento19 páginasGIGITAN ULAR BERBISA: GEJALA, PENANGANAN DAN JENIS ULAR PALING BERBISAYudhistira ArifAún no hay calificaciones
- Ultra Shred Workout (By Brian Jung)Documento10 páginasUltra Shred Workout (By Brian Jung)sannaluizazampro0100% (1)
- Ecological PyramidsDocumento19 páginasEcological Pyramidsnandhinidish100% (1)
- L Sit ProgramDocumento23 páginasL Sit Programdebo100% (1)
- Appendix - 6 - Site Logistics PlanDocumento16 páginasAppendix - 6 - Site Logistics PlanRamesh BabuAún no hay calificaciones
- MMI4804 Quiz 5Documento16 páginasMMI4804 Quiz 5Ham Mad0% (1)
- L-Sit ProgressionsDocumento2 páginasL-Sit ProgressionsMattAún no hay calificaciones
- Skema Jawapan Gerak Gempur 1Documento5 páginasSkema Jawapan Gerak Gempur 1Cikgu RoshailaAún no hay calificaciones
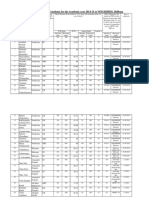
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Documento10 páginasAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaAún no hay calificaciones
- Bcspca Factsheet Life of An Egg Laying Hen PDFDocumento2 páginasBcspca Factsheet Life of An Egg Laying Hen PDFAnonymous 2OMEDZeqCDAún no hay calificaciones
- Sdera Demo Lesson DVD Worksheet 2021Documento2 páginasSdera Demo Lesson DVD Worksheet 2021api-396577001Aún no hay calificaciones
- A Case of Eclectic Family TherapyDocumento88 páginasA Case of Eclectic Family Therapygun gorAún no hay calificaciones
- Community and Public Health DefinitionsDocumento3 páginasCommunity and Public Health DefinitionsSheralyn PelayoAún no hay calificaciones
- Nursing Interventions for Ineffective Airway ClearanceDocumento3 páginasNursing Interventions for Ineffective Airway Clearanceaurezea100% (3)
- Wto Unit-2Documento19 páginasWto Unit-2Anwar KhanAún no hay calificaciones
- Speaking Level Placement Test Business English PDFDocumento2 páginasSpeaking Level Placement Test Business English PDFLee HarrisonAún no hay calificaciones
- 4400 SystemDocumento24 páginas4400 SystemRaniel Aris LigsayAún no hay calificaciones
- Chapter 9 - Managing Crises and National EmergenciesDocumento26 páginasChapter 9 - Managing Crises and National EmergenciesJayson TasarraAún no hay calificaciones
- Hypertension Drugs Cheat Sheet: by ViaDocumento3 páginasHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharAún no hay calificaciones
- Pediatric Malignant Bone TumoursDocumento28 páginasPediatric Malignant Bone TumourscorneliusAún no hay calificaciones
- Maturity-Onset Diabetes of The Young (MODY) : Genetic and Clinical CharacteristicsDocumento5 páginasMaturity-Onset Diabetes of The Young (MODY) : Genetic and Clinical CharacteristicsSarah AgustinAún no hay calificaciones
- The Real Paul Thibault: Nothing But The Truth..Documento20 páginasThe Real Paul Thibault: Nothing But The Truth..LancasterFirstAún no hay calificaciones
- Resolve Family Drainage CatetherDocumento16 páginasResolve Family Drainage CatetherradeonunAún no hay calificaciones
- PE GCSE Revision Quiz - Updated With AnswersDocumento40 páginasPE GCSE Revision Quiz - Updated With AnswersmohitAún no hay calificaciones
- Intro To MycologyDocumento8 páginasIntro To Mycologycamille chuaAún no hay calificaciones
- Syllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsDocumento6 páginasSyllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsOEAEAún no hay calificaciones