También podría gustarte
- Living on the Frontline of COVID-19 in MCO And CMCODe EverandLiving on the Frontline of COVID-19 in MCO And CMCOAún no hay calificaciones
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementDe EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementAún no hay calificaciones
- 2010 PPS Guidelines On DengueDocumento15 páginas2010 PPS Guidelines On DengueOktavian Rizki IlahiAún no hay calificaciones
- Cpm15th Dengue Fever (Doh)Documento18 páginasCpm15th Dengue Fever (Doh)Marko ParungoAún no hay calificaciones
- National Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Adults - Sri LankaDocumento49 páginasNational Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Adults - Sri LankaNational Dengue Control Unit,Sri LankaAún no hay calificaciones
- CPG Dengue - PaediatricDocumento28 páginasCPG Dengue - PaediatricTzeyong FooAún no hay calificaciones
- PCH 32 s1 033Documento6 páginasPCH 32 s1 033dydy_7193Aún no hay calificaciones
- CPG Management of Dengue Infection in Adults (Revised 2nd Edition)Documento68 páginasCPG Management of Dengue Infection in Adults (Revised 2nd Edition)umiraihana1Aún no hay calificaciones
- Dengue ClassificationDocumento11 páginasDengue ClassificationzhafranAún no hay calificaciones
- National Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaDocumento53 páginasNational Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaNational Dengue Control Unit,Sri Lanka100% (1)
- Pang Et Al 2014Documento11 páginasPang Et Al 2014paiskopaxiew888Aún no hay calificaciones
- Management of - Dengue Fever in ChildrenDocumento27 páginasManagement of - Dengue Fever in Childrenumiraihana1Aún no hay calificaciones
- Guidelines For The Management of DF and DHF in AdultsDocumento46 páginasGuidelines For The Management of DF and DHF in AdultsNanda SulistyaningrumAún no hay calificaciones
- Dengue How ClassifyDocumento5 páginasDengue How ClassifyErlin IrawatiAún no hay calificaciones
- Management of Dengue Fever in Children PDFDocumento41 páginasManagement of Dengue Fever in Children PDFnakalnakal2015Aún no hay calificaciones
- Cpm15th Dengue Fever (Doh)Documento18 páginasCpm15th Dengue Fever (Doh)Jeanne Marie ValesAún no hay calificaciones
- Dengue GCP GuidelinesDocumento127 páginasDengue GCP GuidelinesShafiq AhmadAún no hay calificaciones
- Algorithms For The Clinical Management of Dengue Patients (2020)Documento16 páginasAlgorithms For The Clinical Management of Dengue Patients (2020)Charlie CharcapeAún no hay calificaciones
- 2020 Cde Algorithms Dengue Regional enDocumento16 páginas2020 Cde Algorithms Dengue Regional endr FaisalAún no hay calificaciones
- Dengue Guideline 082012 Edit UmyDocumento47 páginasDengue Guideline 082012 Edit UmyFarika NorAún no hay calificaciones
- 671 - Rhinosinusitis and Nasal Polyps (CompleteDocumento89 páginas671 - Rhinosinusitis and Nasal Polyps (CompleteAprilla Handayani100% (1)
- JBB2012 151967Documento13 páginasJBB2012 151967Prodia Central Java RegionAún no hay calificaciones
- 4550 16204 1 PBDocumento7 páginas4550 16204 1 PBKhoirunisah Dwi HartantiAún no hay calificaciones
- Manual of Procedures NTP 5th EditionDocumento172 páginasManual of Procedures NTP 5th EditionMercuryCas100% (3)
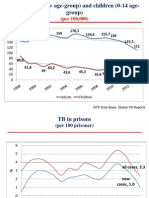
- NTP Data Base. Global TB ReportsDocumento36 páginasNTP Data Base. Global TB ReportsComingSoonAún no hay calificaciones
- TB Bahasa 11-15Documento5 páginasTB Bahasa 11-15MomonAún no hay calificaciones
- Anak Bu HeniDocumento10 páginasAnak Bu HeniVeronika IntanAún no hay calificaciones
- COVID-19: Who To Test and When? CME / ABIM MOC / CEDocumento6 páginasCOVID-19: Who To Test and When? CME / ABIM MOC / CELuis Henrique SalesAún no hay calificaciones
- 2016 Article 1849 PDFDocumento8 páginas2016 Article 1849 PDFdydy_7193Aún no hay calificaciones
- National Tuberculosis Program MOPDocumento192 páginasNational Tuberculosis Program MOPlpanatalioAún no hay calificaciones
- Ypgh 113 1695081Documento12 páginasYpgh 113 1695081Pawan MishraAún no hay calificaciones
- Definitive Tests For Dengue Fever When and Which SDocumento5 páginasDefinitive Tests For Dengue Fever When and Which SAlone EvensAún no hay calificaciones
- PCAP UpdatesDocumento60 páginasPCAP UpdatesMarko ParungoAún no hay calificaciones
- Information For Laboratories About Coronavirus Diagnosis TestDocumento11 páginasInformation For Laboratories About Coronavirus Diagnosis Testمحمد علي حريج / مسائيAún no hay calificaciones
- Report of National Consultation On Diagnosis and Treatment of Pediatric TBDocumento27 páginasReport of National Consultation On Diagnosis and Treatment of Pediatric TBArun GeorgeAún no hay calificaciones
- Typhoid & Paratyphoid Fever Investigation GuideDocumento16 páginasTyphoid & Paratyphoid Fever Investigation Guidegandes winarniAún no hay calificaciones
- NTCP MOP 5e FinalDocumento192 páginasNTCP MOP 5e FinalcharmainegoAún no hay calificaciones
- 2nd Edition of Malaysian COPD Clinical Practice GuidelineDocumento67 páginas2nd Edition of Malaysian COPD Clinical Practice GuidelineFay Fanny FlanneryAún no hay calificaciones
- Medical Care Organization To Face Dengue EpidemicsDocumento12 páginasMedical Care Organization To Face Dengue EpidemicsDAVIDSERGIO39946Aún no hay calificaciones
- Consensus StatementDocumento4 páginasConsensus StatementPrasanna NarayananAún no hay calificaciones
- Case Definitions For Infectious Diseases in Malaysia 2nd Edition Jan 2006Documento110 páginasCase Definitions For Infectious Diseases in Malaysia 2nd Edition Jan 2006Veronica Vivi67% (3)
- TRZ 068Documento8 páginasTRZ 068salsabilapraninditaAún no hay calificaciones
- Diagnosis and Treatment of Chronic CoughDe EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoAún no hay calificaciones
- Living on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19De EverandLiving on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19Aún no hay calificaciones
- Guidance for COVID-19: Prevention, Control, Diagnosis and ManagementDe EverandGuidance for COVID-19: Prevention, Control, Diagnosis and ManagementAún no hay calificaciones
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19De EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19Aún no hay calificaciones
- Atopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseDe EverandAtopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseCalificación: 5 de 5 estrellas5/5 (1)
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?De EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?Aún no hay calificaciones
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsDe EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsAún no hay calificaciones
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingDe EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingAún no hay calificaciones
- Nursing care process in patients with chronic obstructive pulmonary diseaseDe EverandNursing care process in patients with chronic obstructive pulmonary diseaseAún no hay calificaciones
- Hypertension and 24-hour Ambulatory Blood Pressure MonitoringDe EverandHypertension and 24-hour Ambulatory Blood Pressure MonitoringAún no hay calificaciones
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareDe EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareAún no hay calificaciones
- China's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19De EverandChina's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19Aún no hay calificaciones