También podría gustarte
- Applicationb IIDocumento7 páginasApplicationb IIreload99Aún no hay calificaciones
- AA - App FillableDocumento6 páginasAA - App FillableMucyo Rutagengwa KennAún no hay calificaciones
- Registration PacketDocumento4 páginasRegistration PacketStoweRecreationAún no hay calificaciones
- London Kids Admn Form - CDRDocumento4 páginasLondon Kids Admn Form - CDRDeeniyat ChanserpurAún no hay calificaciones
- Allen County Board of DD Student Emergency DataDocumento2 páginasAllen County Board of DD Student Emergency Dataadhi eng lrtAún no hay calificaciones
- B.TH M.div Application NLBCDocumento11 páginasB.TH M.div Application NLBCprinceforjesusAún no hay calificaciones
- T-Shirt Size (Adult Sizes) Xs SM Med LG XL XXLDocumento3 páginasT-Shirt Size (Adult Sizes) Xs SM Med LG XL XXLmainstageAún no hay calificaciones
- Registration FormDocumento2 páginasRegistration FormAlex Maverick WhittakerAún no hay calificaciones
- 2012 Child Care Services Branch Youth Information FormDocumento5 páginas2012 Child Care Services Branch Youth Information FormymcawncAún no hay calificaciones
- Registration Form: Choose Your ProgramDocumento1 páginaRegistration Form: Choose Your ProgramJoins 세계유학Aún no hay calificaciones
- ASYMCAreg Summercamp2011Documento2 páginasASYMCAreg Summercamp2011ASYMCA YCOAún no hay calificaciones
- NMTC-Application-Form-Final (1)Documento5 páginasNMTC-Application-Form-Final (1)icttumainiAún no hay calificaciones
- Rady Childrens HospitalDocumento6 páginasRady Childrens HospitalTom HeavenAún no hay calificaciones
- MKU Internal Scholarship Application Form 2022Documento9 páginasMKU Internal Scholarship Application Form 2022Nchoe StephenAún no hay calificaciones
- Summer Volunteer ApplicationDocumento4 páginasSummer Volunteer ApplicationtymkidsAún no hay calificaciones
- NUST Surety Bond for StudentsDocumento2 páginasNUST Surety Bond for StudentsHamza SehgalAún no hay calificaciones
- Prenatal Req PDFDocumento4 páginasPrenatal Req PDFVARDHINI N V RAMA JOGARAOAún no hay calificaciones
- History Form For AdultsDocumento9 páginasHistory Form For AdultsFazal HaqueAún no hay calificaciones
- CampmsghealthformDocumento1 páginaCampmsghealthformapi-317400714Aún no hay calificaciones
- Brain Train Is 2015Documento2 páginasBrain Train Is 2015scribdlertooAún no hay calificaciones
- Teen MedicalDocumento1 páginaTeen MedicalJohn C StarkAún no hay calificaciones
- Adult Case History Form2Documento6 páginasAdult Case History Form2Josè Miguel Amador SantibañezAún no hay calificaciones
- Brother and Sister:: Scholarships and Financial Assistance Division Office of Student Affairs UPLB, College, LagunaDocumento2 páginasBrother and Sister:: Scholarships and Financial Assistance Division Office of Student Affairs UPLB, College, LagunaAnnabella LacunaAún no hay calificaciones
- Oil and Gas Scholarship Application DeadlineDocumento5 páginasOil and Gas Scholarship Application Deadlineee0785Aún no hay calificaciones
- ADM-FR-003 Student Directory FormDocumento2 páginasADM-FR-003 Student Directory FormRahayuAún no hay calificaciones
- Distinction College Application Form 1Documento2 páginasDistinction College Application Form 1Charlene LoveAún no hay calificaciones
- Admission Form Format - Draft 2016Documento4 páginasAdmission Form Format - Draft 2016Chaitanya MullapudiAún no hay calificaciones
- Little Lambs Preschool Application FormDocumento12 páginasLittle Lambs Preschool Application FormNoopur JainAún no hay calificaciones
- Beaconhouse Academic Scholarship Application Form: Recent Passport Sized PhotographDocumento2 páginasBeaconhouse Academic Scholarship Application Form: Recent Passport Sized Photographsyed qasim bukhariAún no hay calificaciones
- Learning Camp RegistrationDocumento1 páginaLearning Camp RegistrationAaron James LicoAún no hay calificaciones
- Summer Camp ApplicationDocumento8 páginasSummer Camp ApplicationRocio BarrioAún no hay calificaciones
- PDS - 2022-2023 PDFDocumento2 páginasPDS - 2022-2023 PDFMarcelino CalataAún no hay calificaciones
- Foster ApplicationDocumento2 páginasFoster ApplicationGina HobbsAún no hay calificaciones
- Registration and WaiverDocumento1 páginaRegistration and WaiverbradenandcheriAún no hay calificaciones
- Employment / Job Application: Page 1 of 4Documento4 páginasEmployment / Job Application: Page 1 of 4api-545870588Aún no hay calificaciones
- Appletree NP Forms FillableDocumento2 páginasAppletree NP Forms FillableFabian SvrAún no hay calificaciones
- J-K Student ApplicationDocumento3 páginasJ-K Student Applicationallandog06Aún no hay calificaciones
- Adult Health HistoryDocumento1 páginaAdult Health HistorySally Hansen100% (1)
- Registration Form For PDO's 2018Documento5 páginasRegistration Form For PDO's 2018Catherine Christine HarrisAún no hay calificaciones
- Order FormDocumento2 páginasOrder Formrmckenzie7811Aún no hay calificaciones
- Registration FormDocumento3 páginasRegistration FormFayetoot IgnAún no hay calificaciones
- SCA Application Admission 2021 StudentDocumento3 páginasSCA Application Admission 2021 StudentJavan SmithAún no hay calificaciones
- Counseling and Testing ServicesDocumento3 páginasCounseling and Testing ServicesTuTitAún no hay calificaciones
- General Release / Permission Form: ACTIVITIES: (Initial All That Apply)Documento2 páginasGeneral Release / Permission Form: ACTIVITIES: (Initial All That Apply)Megan JonesAún no hay calificaciones
- Canine Connections of NC Dog Adoption Application Form: Contact InformationDocumento5 páginasCanine Connections of NC Dog Adoption Application Form: Contact InformationMaria C DenningAún no hay calificaciones
- AVI Application FormDocumento3 páginasAVI Application FormAding PanganuronAún no hay calificaciones
- Elm-Application Intensive 2011Documento2 páginasElm-Application Intensive 2011jchunter22Aún no hay calificaciones
- PL XC Parent Permission Slip 2022Documento1 páginaPL XC Parent Permission Slip 2022mjdelmiguez05Aún no hay calificaciones
- NBS & Discharge Plan (New)Documento3 páginasNBS & Discharge Plan (New)Aina HaravataAún no hay calificaciones
- Registration Forms 2024Documento2 páginasRegistration Forms 2024api-276553863Aún no hay calificaciones
- HVL ApplicationDocumento3 páginasHVL Application56hrsw2qb8Aún no hay calificaciones
- ADM-FR-003 Student Directory Form (To Be Accomplished by Qualified App)Documento2 páginasADM-FR-003 Student Directory Form (To Be Accomplished by Qualified App)Lyra Mae Belista MaravillaAún no hay calificaciones
- St. George AppDocumento9 páginasSt. George AppFutureDDSAún no hay calificaciones
- Texas Bible Institute: SECTION A - General InformationDocumento12 páginasTexas Bible Institute: SECTION A - General InformationBrute1989Aún no hay calificaciones
- Griffin Observership ApplicationDocumento7 páginasGriffin Observership Applicationসোমনাথ মহাপাত্রAún no hay calificaciones
- 2019 Summer Youth Camp: Christian Youth Fellowship Westside of Burnham Park, Baguio CityDocumento1 página2019 Summer Youth Camp: Christian Youth Fellowship Westside of Burnham Park, Baguio CityTitus ScribeAún no hay calificaciones
- 2015 Ski Venture Booking FormDocumento2 páginas2015 Ski Venture Booking FormdustersAún no hay calificaciones
- Progressive Health Care: Critical Health Care InformationDe EverandProgressive Health Care: Critical Health Care InformationAún no hay calificaciones
- The Honest and Direct Truth to Resumes from an HR Director PerspectiveDe EverandThe Honest and Direct Truth to Resumes from an HR Director PerspectiveAún no hay calificaciones
- IQRA ACADEMY O LEVELS MID TERM EXAMS MATHDocumento9 páginasIQRA ACADEMY O LEVELS MID TERM EXAMS MATHWaseem AhmedAún no hay calificaciones
- Chapter 4 Lecture 1Documento4 páginasChapter 4 Lecture 1Waseem AhmedAún no hay calificaciones
- Algebraic Expression Forming Algebraic ExpressionDocumento4 páginasAlgebraic Expression Forming Algebraic ExpressionWaseem AhmedAún no hay calificaciones
- Maths MsDocumento2 páginasMaths MsWaseem AhmedAún no hay calificaciones
- Chapter 5.1Documento2 páginasChapter 5.1Waseem AhmedAún no hay calificaciones
- Superposition of Waves 1Documento4 páginasSuperposition of Waves 1Waseem AhmedAún no hay calificaciones
- Unit 1 - Cell Structure and Organisation Without Slide Prep BackupDocumento9 páginasUnit 1 - Cell Structure and Organisation Without Slide Prep BackupWaseem AhmedAún no hay calificaciones
- Unit 3 - EnzymesDocumento5 páginasUnit 3 - EnzymesWaseem AhmedAún no hay calificaciones
- Unit 2 - Diffussion and OsmosisDocumento9 páginasUnit 2 - Diffussion and OsmosisWaseem AhmedAún no hay calificaciones
- Chapter 5.1Documento2 páginasChapter 5.1Waseem AhmedAún no hay calificaciones
- Worksheet Plant NutritionDocumento2 páginasWorksheet Plant NutritionWaseem AhmedAún no hay calificaciones
- AS Physics NotesDocumento6 páginasAS Physics NotesWaseem AhmedAún no hay calificaciones
- Iqra Academy Abbottabad Mats PaperDocumento8 páginasIqra Academy Abbottabad Mats PaperWaseem AhmedAún no hay calificaciones
- Vectors Basic WorksheetDocumento1 páginaVectors Basic WorksheetWaseem AhmedAún no hay calificaciones
- Charged Particles Magnetic FieldsDocumento10 páginasCharged Particles Magnetic FieldsWaseem AhmedAún no hay calificaciones
- Chapter 6Documento2 páginasChapter 6Waseem AhmedAún no hay calificaciones
- Wave 1Documento6 páginasWave 1Waseem AhmedAún no hay calificaciones
- Chapter 5.1Documento2 páginasChapter 5.1Waseem AhmedAún no hay calificaciones
- Paper 1mcqsDocumento2 páginasPaper 1mcqsWaseem AhmedAún no hay calificaciones
- PaperDocumento11 páginasPaperWaseem AhmedAún no hay calificaciones
- Flashing LED Project: Parts RequiredDocumento1 páginaFlashing LED Project: Parts RequiredWaseem AhmedAún no hay calificaciones
- 2 Atoms, Molecules and Stoichiometry PDFDocumento10 páginas2 Atoms, Molecules and Stoichiometry PDFWaseem AhmedAún no hay calificaciones
- University of Cambridge International Examinations General CertificateDocumento8 páginasUniversity of Cambridge International Examinations General CertificateHubbak KhanAún no hay calificaciones
- Mocks Paper 1Documento17 páginasMocks Paper 1Waseem AhmedAún no hay calificaciones
- Chapter: Standing Waves 13-12-2016: Objective 1Documento2 páginasChapter: Standing Waves 13-12-2016: Objective 1Waseem AhmedAún no hay calificaciones
- Position VectorDocumento29 páginasPosition VectorWaseem AhmedAún no hay calificaciones
- Lecture 2Documento3 páginasLecture 2Waseem AhmedAún no hay calificaciones
- AS Economics Guide to Key ConceptsDocumento57 páginasAS Economics Guide to Key ConceptsprayashkAún no hay calificaciones
- Topic 5Documento9 páginasTopic 5Waseem AhmedAún no hay calificaciones
- Iqra Academy Abbottabad: Biology Assessment: Topic: Transport in AnimalDocumento4 páginasIqra Academy Abbottabad: Biology Assessment: Topic: Transport in AnimalWaseem AhmedAún no hay calificaciones
- Chapter 4 Financial AssetsDocumento54 páginasChapter 4 Financial AssetsAddisalem MesfinAún no hay calificaciones
- Tally - ERP9 Online Training: About This CourseDocumento3 páginasTally - ERP9 Online Training: About This CoursePrasenjit SahaAún no hay calificaciones
- Key Blockchain ConceptsDocumento6 páginasKey Blockchain ConceptsMadu AlexAún no hay calificaciones
- ReportsDocumento3 páginasReportsashish sharmaAún no hay calificaciones
- Clayton's CaseDocumento2 páginasClayton's CaseMiscellaneous100% (1)
- Sabastina EllingsworthDocumento2 páginasSabastina Ellingsworthapi-381843241Aún no hay calificaciones
- Retail Technology Guide 2017Documento157 páginasRetail Technology Guide 2017Mike EdwardsAún no hay calificaciones
- Overview of SAP ISRDocumento18 páginasOverview of SAP ISRGOVINDRAJAún no hay calificaciones
- Bank UndertakingDocumento3 páginasBank UndertakingMuhammad YunusAún no hay calificaciones
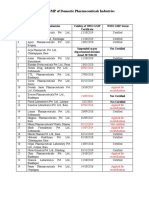
- Status of Nepali Pharma GMP CertificationDocumento2 páginasStatus of Nepali Pharma GMP CertificationDapper Yourself100% (1)
- Invoice 41071Documento2 páginasInvoice 41071Zinhle MpofuAún no hay calificaciones
- Tally Spss PDFDocumento42 páginasTally Spss PDFAkshay PoplyAún no hay calificaciones
- Ret 23Documento2 páginasRet 23sreedev sureshbabuAún no hay calificaciones
- Banking Law Practice Questions and Answers 2Documento4 páginasBanking Law Practice Questions and Answers 2Phetho MachiliAún no hay calificaciones
- Managerial Accounting Braun 4th Edition Solutions ManualDocumento7 páginasManagerial Accounting Braun 4th Edition Solutions Manualbarrenlywale1ibn8Aún no hay calificaciones
- E StatementDocumento4 páginasE StatementMuhammad Basit Mujahid. 105Aún no hay calificaciones
- Trade PayablesDocumento2 páginasTrade PayablesMeghaAún no hay calificaciones
- Source Documents NotesDocumento12 páginasSource Documents NotesStephen mgongolwaAún no hay calificaciones
- Incoterms 1Documento16 páginasIncoterms 1BalasubramanianAún no hay calificaciones
- ERP Systems: Production and Materials Management: Enterprise Resource Planning, 1 Edition by Mary SumnerDocumento21 páginasERP Systems: Production and Materials Management: Enterprise Resource Planning, 1 Edition by Mary Sumnerniceneha_nehaAún no hay calificaciones
- Hospitals Patient Care Units and Ward ManagementDocumento22 páginasHospitals Patient Care Units and Ward Managementsaritatelma78% (41)
- Quality and Safety Synthesis PaperDocumento6 páginasQuality and Safety Synthesis Paperapi-252807964Aún no hay calificaciones
- Assignment Comper ProblemDocumento2 páginasAssignment Comper ProblemAmir ParwarishAún no hay calificaciones
- DSMM 1Documento22 páginasDSMM 1kisam78442Aún no hay calificaciones
- Mt103 Deutsche Bank 500euroDocumento2 páginasMt103 Deutsche Bank 500eurorasool mehrjoo100% (1)
- QuizletDocumento4 páginasQuizletKizzea Bianca GadotAún no hay calificaciones
- Statement of Axis Account No:914010048627688 For The Period (From: 20-12-2020 To: 18-01-2021)Documento2 páginasStatement of Axis Account No:914010048627688 For The Period (From: 20-12-2020 To: 18-01-2021)karanAún no hay calificaciones
- A Project Report On "Lic Housing Finance Loan"Documento14 páginasA Project Report On "Lic Housing Finance Loan"Nia SharmaAún no hay calificaciones
- ACCT 1 - Ch.7Documento13 páginasACCT 1 - Ch.7HIEP PHAM HOANGAún no hay calificaciones
- Role of information systems in tourismDocumento18 páginasRole of information systems in tourismMir AqibAún no hay calificaciones