También podría gustarte
- Assessment of the Politraumatized PatientDe EverandAssessment of the Politraumatized PatientAún no hay calificaciones
- Iii. Physical Assessment and Review of SystemDocumento7 páginasIii. Physical Assessment and Review of SystemBiya MacunteAún no hay calificaciones
- OB Patho Assessment Tool EditedDocumento6 páginasOB Patho Assessment Tool EditedDarren RobertoAún no hay calificaciones
- Preparation Worksheets For NUR 345 Heart Failure SimDocumento14 páginasPreparation Worksheets For NUR 345 Heart Failure SimclarimerAún no hay calificaciones
- 2 Abdomen Checklist 1Documento3 páginas2 Abdomen Checklist 1Angela DancelAún no hay calificaciones
- 01 Nursing Note SampleDocumento1 página01 Nursing Note Sampletesttest testAún no hay calificaciones
- Care PlanDocumento11 páginasCare PlanCathy GewontAún no hay calificaciones
- Physician EvaluationDocumento6 páginasPhysician Evaluationbartoncreekal100% (2)
- Cagayan de Oro City College of Nursing Assessment Form General InformationDocumento11 páginasCagayan de Oro City College of Nursing Assessment Form General Informationdjanggo18Aún no hay calificaciones
- Tgs Ibu Ellen 1Documento11 páginasTgs Ibu Ellen 1rosna wallyAún no hay calificaciones
- Case Study (Iph) Amoebiasis Diarrhea With Mild DHNDocumento9 páginasCase Study (Iph) Amoebiasis Diarrhea With Mild DHNLance_Joshua_7907Aún no hay calificaciones
- Clinical Pathway For Hypertensive Urgency (Revised)Documento6 páginasClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarAún no hay calificaciones
- Tgas Ibu LlenDocumento10 páginasTgas Ibu LlenFifi FebriantiAún no hay calificaciones
- Case-Study-2 AsthmaDocumento5 páginasCase-Study-2 Asthmaangelica dizon100% (1)
- Telemetry Recognition WorkbookDocumento29 páginasTelemetry Recognition WorkbookQueenAún no hay calificaciones
- Complete COVID AdmissionVentilation Decision Tree Formatted 1Documento4 páginasComplete COVID AdmissionVentilation Decision Tree Formatted 1Beauty NightlymareAún no hay calificaciones
- BlehDocumento3 páginasBlehkula diamondAún no hay calificaciones
- Last CareplanDocumento22 páginasLast CareplanNneka Adaeze AnyanwuAún no hay calificaciones
- Nursing Care Plan Example NR450Documento8 páginasNursing Care Plan Example NR450J15Aún no hay calificaciones
- Nursing Concept Map 1Documento3 páginasNursing Concept Map 1Norah Okafor Ezike67% (3)
- Heath Assessment ToolDocumento8 páginasHeath Assessment ToolHouda Hayek100% (1)
- Labor Room and NurseryDocumento2 páginasLabor Room and NurseryLecery Sophia WongAún no hay calificaciones
- Baystate Med CTR Rapid Response Team Recordwith SBARDocumento3 páginasBaystate Med CTR Rapid Response Team Recordwith SBARDanishyana DhiwaneoAún no hay calificaciones
- Physical AssessmentDocumento51 páginasPhysical AssessmentJasmin Jacob100% (2)
- Diabetic Evaluation (Adults Only) : Form To Be Completed by StudentDocumento2 páginasDiabetic Evaluation (Adults Only) : Form To Be Completed by StudentNabeel ShahzadAún no hay calificaciones
- Case Study Jim SandersonDocumento6 páginasCase Study Jim SandersonJessica McAlexanderAún no hay calificaciones
- Admit OrdersDocumento2 páginasAdmit OrdersTariq Niaz Ahmad, MDAún no hay calificaciones
- P.A. Tool (Case Pres FINAL.)Documento23 páginasP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonAún no hay calificaciones
- 2.physical E, HISTORY NCPDocumento13 páginas2.physical E, HISTORY NCPمريم حجيAún no hay calificaciones
- RevisedDocumento16 páginasRevisedZymer Lee AbasoloAún no hay calificaciones
- Neuro AssessmentDocumento42 páginasNeuro AssessmentLydia Lopz MsnrncdAún no hay calificaciones
- Nursing Care Plan PackageCDocumento23 páginasNursing Care Plan PackageCralsadat100% (1)
- (193213049) Putu Riska Pramudita DewiDocumento10 páginas(193213049) Putu Riska Pramudita DewiDianAún no hay calificaciones
- Intestnal ObstructionDocumento4 páginasIntestnal ObstructionRenea Joy ArruejoAún no hay calificaciones
- ChartingDocumento3 páginasChartingLorina Lynne ApelacioAún no hay calificaciones
- Head-To-Toe Checklist: Beautiful Nursing LLCDocumento4 páginasHead-To-Toe Checklist: Beautiful Nursing LLCcarlyAún no hay calificaciones
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocumento20 páginasPharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDzaky UlayyaAún no hay calificaciones
- Mang Kanor ROSDocumento2 páginasMang Kanor ROSChamelli RobinAún no hay calificaciones
- Head To ToeDocumento4 páginasHead To Toenazbeen.ahmadiAún no hay calificaciones
- Care Plan For CHFDocumento9 páginasCare Plan For CHFJon Djchimz IsidroAún no hay calificaciones
- Assessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationDocumento10 páginasAssessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationApol Pen67% (3)
- Welcome To Orthopedics Care Center !Documento2 páginasWelcome To Orthopedics Care Center !Ahmed M. RafatAún no hay calificaciones
- Competency Assessment Exam For Nurses: Qibah Hospital Qibah, Algassim, KsaDocumento4 páginasCompetency Assessment Exam For Nurses: Qibah Hospital Qibah, Algassim, KsaSherina W. Edding100% (1)
- Acute Kidney Failure Assesment FormDocumento5 páginasAcute Kidney Failure Assesment FormAahad AmeenAún no hay calificaciones
- Documentation in Your 3 Year and Beyond: Summer Quarter 2010Documento32 páginasDocumentation in Your 3 Year and Beyond: Summer Quarter 2010Roberto ParedesAún no hay calificaciones
- Nifedipine 30 MG 1tab PO OD : SPS Shaina Sango SN, SJPIICDDocumento17 páginasNifedipine 30 MG 1tab PO OD : SPS Shaina Sango SN, SJPIICDInnocent-j CartagenaAún no hay calificaciones
- Case Study Medical WardDocumento14 páginasCase Study Medical WardJoshAún no hay calificaciones
- Csu, Stanislaus B.S.N. Clinical Plan of Care Patient DataDocumento18 páginasCsu, Stanislaus B.S.N. Clinical Plan of Care Patient Dataapi-284664489Aún no hay calificaciones
- Antepartum Record Labor WatchDocumento4 páginasAntepartum Record Labor WatchMaryJoy rosalesAún no hay calificaciones
- Neri NCP 1Documento4 páginasNeri NCP 1Emmanuel_Neri_3662Aún no hay calificaciones
- Health Examination RecordDocumento4 páginasHealth Examination Recordmary joy dela cruzAún no hay calificaciones
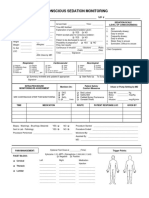
- 34 An Consious Sedation MonitoringDocumento2 páginas34 An Consious Sedation Monitoringabu alauon abed almohsenAún no hay calificaciones
- 1-General ExaminationDocumento5 páginas1-General Examinationalmatrim10Aún no hay calificaciones
- EKONSULTA FormDocumento13 páginasEKONSULTA FormJirhana Lindagan Karon-KampangAún no hay calificaciones
- 05 Nursing Note SampleDocumento3 páginas05 Nursing Note Sampletesttest testAún no hay calificaciones
- Health Screening and Assessment Form - SampleDocumento3 páginasHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Intake and OutputDocumento3 páginasIntake and Outputtina100% (1)
- Post Anaesthesia Recovery ScoreDocumento2 páginasPost Anaesthesia Recovery ScoreRaviraj Pishe50% (2)
- Post Anaesthesia Recovery Score PDFDocumento2 páginasPost Anaesthesia Recovery Score PDFBombay Hospital100% (1)
- Hip FractureDocumento4 páginasHip Fracturemariafub100% (1)
- Prostate Cancer Must Be Differentiated From: (BPH)Documento4 páginasProstate Cancer Must Be Differentiated From: (BPH)Robert StolnicuAún no hay calificaciones
- Transgenic ValidationDocumento22 páginasTransgenic ValidationSyama J.S33% (6)
- Common Diseases in ChildrenDocumento263 páginasCommon Diseases in ChildrenSuneethaVangala100% (1)
- Alliance Physical TherapyDocumento178 páginasAlliance Physical TherapyAlliance Physical Therapy100% (1)
- Blood Transfusion LearningDocumento36 páginasBlood Transfusion LearningHarjotBrarAún no hay calificaciones
- Urine SedimentDocumento38 páginasUrine Sedimentcyrhenmie100% (1)
- Prayer Points: April 2013Documento4 páginasPrayer Points: April 2013doorkeepersAún no hay calificaciones
- AcetylcysteineDocumento2 páginasAcetylcysteineMeriLyn Parayno83% (6)
- Efficacy & Safety Traditional Plant MedicinesDocumento50 páginasEfficacy & Safety Traditional Plant MedicinesRaymond ObomsawinAún no hay calificaciones
- Calprotectin LactoferrinDocumento16 páginasCalprotectin LactoferrinCristian LaraAún no hay calificaciones
- Sdo PM QF Sgod SHN 001 Students Health Card ElementaryDocumento3 páginasSdo PM QF Sgod SHN 001 Students Health Card ElementaryShiela E. EladAún no hay calificaciones
- Fourth Unit-EditedDocumento5 páginasFourth Unit-EditedS. C.Aún no hay calificaciones
- Care of The Clients With Eye and Ear DisorderDocumento35 páginasCare of The Clients With Eye and Ear DisorderKristine Joy RevañoAún no hay calificaciones
- Current Issues in Postoperative Pain Management PDFDocumento12 páginasCurrent Issues in Postoperative Pain Management PDFikm fkunissulaAún no hay calificaciones
- Rectal ExaminationDocumento21 páginasRectal ExaminationAlexandra HornariuAún no hay calificaciones
- Recommendation of 11th Safety Conference, 9.7.13Documento48 páginasRecommendation of 11th Safety Conference, 9.7.13ravimutyamAún no hay calificaciones
- Letter From California Attorney General Xavier BecerraDocumento10 páginasLetter From California Attorney General Xavier BecerraThe Press-Enterprise / pressenterprise.comAún no hay calificaciones
- S&P Pharma Industry Overview - 11252010Documento49 páginasS&P Pharma Industry Overview - 11252010earajesh100% (1)
- Answers and Rationale Medical Surgical Nursing Practice Test Part 3Documento4 páginasAnswers and Rationale Medical Surgical Nursing Practice Test Part 3Anna Marie AmpoAún no hay calificaciones
- Abdominal X RayDocumento45 páginasAbdominal X RayAbdullah As'adAún no hay calificaciones
- CDXDocumento5 páginasCDXJessa BorreAún no hay calificaciones
- Rheumatoid ArthritisDocumento14 páginasRheumatoid ArthritisLorebell100% (5)
- Amritacon Schedule PDFDocumento7 páginasAmritacon Schedule PDFShrinivas YuvanAún no hay calificaciones
- Rujukan Feb 2021Documento11 páginasRujukan Feb 2021yela zAún no hay calificaciones
- An Interview With Dr. Rudi Moerck On Prostate Health by Dr. MercolaDocumento13 páginasAn Interview With Dr. Rudi Moerck On Prostate Health by Dr. Mercolaalekad65100% (1)
- Art15 PDFDocumento6 páginasArt15 PDFNatalia TexidorAún no hay calificaciones
- Perichondritis - Not Just Simple Cellulitis - REBEL EM - Emergency Medicine BlogDocumento8 páginasPerichondritis - Not Just Simple Cellulitis - REBEL EM - Emergency Medicine BlogMarica SibulovAún no hay calificaciones
- 12.ficus HispidaDocumento5 páginas12.ficus HispidaBaru Chandrasekhar RaoAún no hay calificaciones
- A Guide To Clinical Differential Diagnosis PDFDocumento41 páginasA Guide To Clinical Differential Diagnosis PDFNisa Nafiah OktavianiAún no hay calificaciones