También podría gustarte
- Modification of Dental Treatment HandoutDocumento7 páginasModification of Dental Treatment HandoutnewmexicoomfsAún no hay calificaciones
- The ADA Practical Guide to Patients with Medical ConditionsDe EverandThe ADA Practical Guide to Patients with Medical ConditionsAún no hay calificaciones
- Fixed Orthodontic Appliances: A Practical GuideDe EverandFixed Orthodontic Appliances: A Practical GuideCalificación: 1 de 5 estrellas1/5 (1)
- Management of Medically Compromised PatientsDocumento70 páginasManagement of Medically Compromised PatientsPriyanka WadhawanAún no hay calificaciones
- Medically Compromised PatientsDocumento21 páginasMedically Compromised PatientsDyah Wulan RamadhaniAún no hay calificaciones
- OSCE Pediatric Dentistry Lecture-AnswersDocumento40 páginasOSCE Pediatric Dentistry Lecture-AnswersR MAún no hay calificaciones
- Antibiotics Used in DentistryDocumento17 páginasAntibiotics Used in Dentistrymegamarwa50% (2)
- Essential Tissue Healing of the Face and NeckDe EverandEssential Tissue Healing of the Face and NeckCalificación: 5 de 5 estrellas5/5 (2)
- Management of Medically Compromised Orthodontic PatientsDocumento64 páginasManagement of Medically Compromised Orthodontic Patientsakshi1947Aún no hay calificaciones
- IRTDocumento2 páginasIRTIgnacioAún no hay calificaciones
- A Guide To Succeeding in The Df1 Interview (Sample Pages Only)Documento15 páginasA Guide To Succeeding in The Df1 Interview (Sample Pages Only)jaipald9067% (3)
- Classification of Periodontal Diseases and Conditions 2018Documento15 páginasClassification of Periodontal Diseases and Conditions 2018Jean DatorAún no hay calificaciones
- Pediatric Restorative DentistryDocumento13 páginasPediatric Restorative DentistryKhaled SelimAún no hay calificaciones
- Geriatric Restorative CareDocumento12 páginasGeriatric Restorative CareCeza CezaaAún no hay calificaciones
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionDe EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionAún no hay calificaciones
- Denture Related StomatitisDocumento8 páginasDenture Related StomatitisLike OliviaAún no hay calificaciones
- Evidence Based Management Third MolarsDocumento73 páginasEvidence Based Management Third MolarsCiutac ŞtefanAún no hay calificaciones
- MdsDocumento356 páginasMdsARJUN SreenivasAún no hay calificaciones
- Sorting Out Endodontic Symptoms: ©JK Mitchell, DDS, Med April 2012Documento2 páginasSorting Out Endodontic Symptoms: ©JK Mitchell, DDS, Med April 2012sao_tren_troi100% (1)
- Vital Therapy in Carious ToothDocumento9 páginasVital Therapy in Carious ToothAsh PeiAún no hay calificaciones
- Dental Management For Medically Compromised Patient: Anemia, Sickle Cell Anemia, Thalassemia and G6PDDocumento26 páginasDental Management For Medically Compromised Patient: Anemia, Sickle Cell Anemia, Thalassemia and G6PDAhmad Badruddin100% (3)
- Oral Wound Healing: Cell Biology and Clinical ManagementDe EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaAún no hay calificaciones
- Dental Extractions and Bisphosphonates: The Assess-Ment, Consent and Management, A Proposed AlgorithmDocumento6 páginasDental Extractions and Bisphosphonates: The Assess-Ment, Consent and Management, A Proposed Algorithmdent12Aún no hay calificaciones
- Fixed Clinic Manual 2017Documento74 páginasFixed Clinic Manual 2017Khizer's MusicAún no hay calificaciones
- Atraumatic Tooth ExtractionDocumento10 páginasAtraumatic Tooth ExtractionAnderson AraujoAún no hay calificaciones
- Epidemiologi Dental CariesDocumento21 páginasEpidemiologi Dental CariesSampahAjaAún no hay calificaciones
- Australian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryDocumento7 páginasAustralian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryVishakha SabooAún no hay calificaciones
- Stainless Steel Crowns (SSCS)Documento24 páginasStainless Steel Crowns (SSCS)haneenee0% (1)
- The Single-Tooth RestorationDocumento5 páginasThe Single-Tooth Restorationumerjaved86Aún no hay calificaciones
- Platelet Rich Fibrin in Regenerative Dentistry: Biological Background and Clinical IndicationsDe EverandPlatelet Rich Fibrin in Regenerative Dentistry: Biological Background and Clinical IndicationsRichard J. MironAún no hay calificaciones
- Mucogingival Conditions in The Natural DentitionDocumento10 páginasMucogingival Conditions in The Natural DentitionMartty BaAún no hay calificaciones
- AGGRESSIVE PERIODONTITIS: AN INTRODUCTIONDocumento101 páginasAGGRESSIVE PERIODONTITIS: AN INTRODUCTIONdileep900100% (1)
- Acute Periodontal Conditions: PeriodonticsDocumento9 páginasAcute Periodontal Conditions: Periodonticsmonica896Aún no hay calificaciones
- Root FracturesDocumento9 páginasRoot FracturesAbhilashPadmanabhanAún no hay calificaciones
- Crash Course in Dental Management of The Medically Compromised PatientDocumento30 páginasCrash Course in Dental Management of The Medically Compromised Patientmazen bokhari100% (1)
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDocumento6 páginasEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargAún no hay calificaciones
- Dental Trauma Classification and TreatmentDocumento76 páginasDental Trauma Classification and TreatmentJitender ReddyAún no hay calificaciones
- Mucogingival Surgery Procedures and HealingDocumento46 páginasMucogingival Surgery Procedures and HealingDr.Arshad SayedAún no hay calificaciones
- What Is Root Canal Treatment?Documento2 páginasWhat Is Root Canal Treatment?Vishakha SabooAún no hay calificaciones
- Dental Management of The Patient Undergoing Radiotherapy or ChemoterapyDocumento43 páginasDental Management of The Patient Undergoing Radiotherapy or ChemoterapyJenadi Binarto100% (1)
- Odontogenic Cysts Summary Chart: Radicular Cyst (Periapical Cyst)Documento4 páginasOdontogenic Cysts Summary Chart: Radicular Cyst (Periapical Cyst)ML90Aún no hay calificaciones
- INBDE High-Yield Conditions To KnowDocumento17 páginasINBDE High-Yield Conditions To KnowРами Кальмат100% (1)
- OverdentureDocumento227 páginasOverdentureEazhil RajAún no hay calificaciones
- Intracoronal Attachments For Removable Partial DenturesDocumento18 páginasIntracoronal Attachments For Removable Partial Denturesapi-3710948100% (6)
- Dental Implants Are Contraindicated In...Documento5 páginasDental Implants Are Contraindicated In...Lia DietrichAún no hay calificaciones
- The Risk For Endocarditis in Dental PracticeDocumento9 páginasThe Risk For Endocarditis in Dental PracticeisanreryAún no hay calificaciones
- Extracting Wisdom: Answering the Call to Build High-Impact Oral and Maxillofacial Surgery PracDe EverandExtracting Wisdom: Answering the Call to Build High-Impact Oral and Maxillofacial Surgery PracAún no hay calificaciones
- 2 Extracted Pages From Anna B. Fuks, Benjamin Peretz Eds. Pediatric Endodontics Current Concepts in Pulp Therapy For Primary and Young Permanent TeethDocumento22 páginas2 Extracted Pages From Anna B. Fuks, Benjamin Peretz Eds. Pediatric Endodontics Current Concepts in Pulp Therapy For Primary and Young Permanent TeethMona CameliaAún no hay calificaciones
- CADCAM Vs Traditional Ceramic InlayDocumento10 páginasCADCAM Vs Traditional Ceramic InlayAya Ibrahim YassinAún no hay calificaciones
- Pediatric DentistryDocumento15 páginasPediatric DentistryPeyman Dhg100% (2)
- Dental Considerations-CVS DiseasesDocumento86 páginasDental Considerations-CVS Diseasesapi-3704106100% (1)
- Dental Practicality IndexDocumento4 páginasDental Practicality Indexdorasani99Aún no hay calificaciones
- Comprehensive Periodontal Exam GuideDocumento40 páginasComprehensive Periodontal Exam GuideKavin SandhuAún no hay calificaciones
- Endocrinology (Harriet Lane Handbook) PDFDocumento39 páginasEndocrinology (Harriet Lane Handbook) PDFPancar ChoirAún no hay calificaciones
- Topnotch IM For MoonlightersDocumento274 páginasTopnotch IM For Moonlightersmefav7778520100% (2)
- NCM of Clients With Endocrine DisordersDocumento24 páginasNCM of Clients With Endocrine DisordersArgee Alonsabe100% (1)
- Diagnostic Criteria For Thyroid StormDocumento4 páginasDiagnostic Criteria For Thyroid StormAnonymous ZUaUz1wwAún no hay calificaciones
- Timolol Maleate Ophthalmic Solution, USP 0.25% and 0.5%: Comparative Product InformationDocumento5 páginasTimolol Maleate Ophthalmic Solution, USP 0.25% and 0.5%: Comparative Product InformationNur Utami PakayaAún no hay calificaciones
- Rujukan 2023Documento80 páginasRujukan 2023Dwi Wahyu LestariAún no hay calificaciones
- The First Nursing School in The Philippines: Amie B. Torres Clinical InstructorDocumento35 páginasThe First Nursing School in The Philippines: Amie B. Torres Clinical InstructorAno NymousAún no hay calificaciones
- Hyperthyroidism: Annals of Internal Medicine July 2012Documento17 páginasHyperthyroidism: Annals of Internal Medicine July 2012Deepa RajAún no hay calificaciones
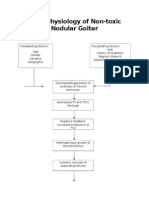
- Pathophysiology of Nontoxic Nodular GoiterDocumento2 páginasPathophysiology of Nontoxic Nodular GoiterJan Jewey80% (10)
- Hyperthyroidism: Case Presentation and DiscussionDocumento7 páginasHyperthyroidism: Case Presentation and DiscussionCalingalan Hussin CaluangAún no hay calificaciones
- Endocrine and Metabolic Disorders PDFDocumento31 páginasEndocrine and Metabolic Disorders PDFAna-Maria50% (2)
- 1Documento28 páginas1Ed Daniel Tanseco DavisAún no hay calificaciones
- How to finish MEDICINE in 1 day: A guide to cardiologyDocumento70 páginasHow to finish MEDICINE in 1 day: A guide to cardiologyshyma shymaAún no hay calificaciones
- Graves' Disease Signs and ManagementDocumento11 páginasGraves' Disease Signs and ManagementManisha Sekaran Muniandy100% (1)
- Enzyme Immunoassay For The Quantitative Determination of Triiodothyronine (T3) in Human SerumDocumento10 páginasEnzyme Immunoassay For The Quantitative Determination of Triiodothyronine (T3) in Human SerumcitrahdynAún no hay calificaciones
- Lab Report NewDocumento2 páginasLab Report Newnsdh5v5v5sAún no hay calificaciones
- Euthrox CharacteristicsDocumento10 páginasEuthrox Characteristicspavaroti37Aún no hay calificaciones
- History ExaminationDocumento18 páginasHistory ExaminationMohammed FaragAún no hay calificaciones
- Foundatios of Evidence Based MedicineDocumento559 páginasFoundatios of Evidence Based MedicineJuan José Ruiz Castillo100% (3)
- Causes and Treatment of DepressionDocumento12 páginasCauses and Treatment of DepressionGEETA MOHANAún no hay calificaciones
- ATA HipertiroidDocumento117 páginasATA HipertiroidjordanAún no hay calificaciones
- What Is Graves' Disease?Documento8 páginasWhat Is Graves' Disease?r4yna_pott3rAún no hay calificaciones
- MRCP Recall May 19Documento10 páginasMRCP Recall May 19Mariam YousifAún no hay calificaciones
- 1 s2.0 S1933287417304403 MainDocumento7 páginas1 s2.0 S1933287417304403 MainSalvador GoveaAún no hay calificaciones
- Endocrinology: SECTION A: Read Each Question Carefully and Record The Answer "TRUE" or "FALSE"Documento9 páginasEndocrinology: SECTION A: Read Each Question Carefully and Record The Answer "TRUE" or "FALSE"Alice TaylorAún no hay calificaciones
- Thyroid and Antityr DrugsDocumento23 páginasThyroid and Antityr Drugsmsmobile shAún no hay calificaciones
- Physiology of The Thyroid GlandDocumento28 páginasPhysiology of The Thyroid GlandSecret AgentAún no hay calificaciones
- Thyroid Stimulating Hormone Test and Its Effect On The Human BodyDocumento4 páginasThyroid Stimulating Hormone Test and Its Effect On The Human BodyInternational Journal of Innovative Science and Research TechnologyAún no hay calificaciones
- 13 - Nuclear 2Documento64 páginas13 - Nuclear 2core radiologyAún no hay calificaciones
- Review Plummer DiseaseDocumento12 páginasReview Plummer DiseaseNovia ChrisnawatiAún no hay calificaciones