También podría gustarte
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Escherichia Coli-A Gram-Negative, Facultative Anaerobic, Rod-Shaped, Coliform Bacterium of The GenusDocumento2 páginasEscherichia Coli-A Gram-Negative, Facultative Anaerobic, Rod-Shaped, Coliform Bacterium of The GenusKent Justin RizonAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5795)
- Pneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsDocumento34 páginasPneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsMenard Velasco100% (1)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- MCQs 1Documento33 páginasMCQs 1Subrahmanyam SudiAún no hay calificaciones
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Largest Organ of The Body IsDocumento10 páginasThe Largest Organ of The Body IsDip Ayan MAún no hay calificaciones
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Kibet Faith JepchirchirDocumento54 páginasKibet Faith JepchirchirSnev EvansAún no hay calificaciones
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- Muhd Yusof V Ahmad WahabDocumento31 páginasMuhd Yusof V Ahmad WahabDheebak KumaranAún no hay calificaciones
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Test Bank For Microbiology A Systems Approach 3rd Edition by CowanDocumento25 páginasTest Bank For Microbiology A Systems Approach 3rd Edition by CowanJoseph Williams100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Etiologic Role of Root Canal Infection in Apical Periodontitis and Its Relationship With Clinical SymptomatologyDocumento29 páginasEtiologic Role of Root Canal Infection in Apical Periodontitis and Its Relationship With Clinical SymptomatologyOmar TalibAún no hay calificaciones
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Universal PrecautionDocumento46 páginasUniversal PrecautionJayrelle D. SafranAún no hay calificaciones
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Common Teratogens and Their EffectsDocumento3 páginasCommon Teratogens and Their EffectsThyataira chuaAún no hay calificaciones
- Mohamad Hamad Infection Control in DentalDocumento25 páginasMohamad Hamad Infection Control in DentalMohamad Hamad100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- CHN - 1Documento23 páginasCHN - 1Raagul SaravanaKumarAún no hay calificaciones
- Parvo BrochureDocumento2 páginasParvo BrochureDumapis RichardAún no hay calificaciones
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Chiron & NAT Introduction KL 29APR08Documento35 páginasChiron & NAT Introduction KL 29APR08api-3750327100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Biorisk Management Basic-Level Materials: TD-O2-009: Biorisk Management Curriculum Development - Academic Track - JordanDocumento26 páginasBiorisk Management Basic-Level Materials: TD-O2-009: Biorisk Management Curriculum Development - Academic Track - JordanMohammad Emad Al MadadhaAún no hay calificaciones
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- CHN Rle Pointers Fixed NotesDocumento6 páginasCHN Rle Pointers Fixed NotesHatdogAún no hay calificaciones
- Covid Prevention and Monitoring System Using Machine LearningDocumento12 páginasCovid Prevention and Monitoring System Using Machine LearningNabiha HasanAún no hay calificaciones
- Covid 19 VocabularyDocumento5 páginasCovid 19 VocabularyAndy08 asAún no hay calificaciones
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- Guidelines On Prevention of Communicable Diseases in Schools Kindergartens Kindergartens Cum Child Care-Centres Child Are CentresDocumento51 páginasGuidelines On Prevention of Communicable Diseases in Schools Kindergartens Kindergartens Cum Child Care-Centres Child Are CentresJam Knows RightAún no hay calificaciones
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
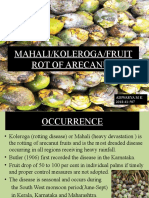
- Mahali/Koleroga/Fruit Rot of Arecanut: Aiswarya M K 2018-41-507Documento16 páginasMahali/Koleroga/Fruit Rot of Arecanut: Aiswarya M K 2018-41-507Aiswarya M KAún no hay calificaciones
- Wing Ho Man (2017) Microbiota of The Respiratory Tract, Gatekeeper To Respiratory HealthDocumento12 páginasWing Ho Man (2017) Microbiota of The Respiratory Tract, Gatekeeper To Respiratory HealthLuan DiasAún no hay calificaciones
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Intro To Epi (Ver. 2)Documento4 páginasIntro To Epi (Ver. 2)Mark Vincent SahagunAún no hay calificaciones
- Hospital Linen ManagementDocumento2 páginasHospital Linen ManagementMarie Paz Lacanlalay Nolasco86% (7)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- WD D-Healthy TravlerDocumento7 páginasWD D-Healthy Travlerapi-285546206Aún no hay calificaciones
- NR442 Community Health Nursing Exam 1 Practice Questions (Instructor Copy)Documento31 páginasNR442 Community Health Nursing Exam 1 Practice Questions (Instructor Copy)carolAún no hay calificaciones
- Sample Case Study BurnDocumento27 páginasSample Case Study BurnRj Cordero75% (4)
- Necrotizing Cellulitis of The Perineum Complicating A Surgical Cure For Bartholinitis: A Case ReportDocumento6 páginasNecrotizing Cellulitis of The Perineum Complicating A Surgical Cure For Bartholinitis: A Case ReportIJAR JOURNALAún no hay calificaciones
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- Class IX Science Why Do We Fall Ill PPT Module 3 - 3Documento17 páginasClass IX Science Why Do We Fall Ill PPT Module 3 - 3Sandeep Kumar100% (2)
- Imci WhoDocumento58 páginasImci WhoCarl Elexer Cuyugan Ano67% (3)
- CHS MCQ Self AssessmentDocumento7 páginasCHS MCQ Self AssessmentDipesh ShresthaAún no hay calificaciones
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)