También podría gustarte
- Hiv/Aids: Mariano Marcos State University College of Health Sciences Department of Nursing Batac City, Ilocos NorteDocumento10 páginasHiv/Aids: Mariano Marcos State University College of Health Sciences Department of Nursing Batac City, Ilocos NorteEyySiEffVee100% (1)
- Interferon Gamma Production in The Course of Mycobacterium Tuberculosis InfectionDocumento9 páginasInterferon Gamma Production in The Course of Mycobacterium Tuberculosis InfectionAndia ReshiAún no hay calificaciones
- Serology Chapter 24 WorksheetDocumento3 páginasSerology Chapter 24 WorksheetRikkiAún no hay calificaciones
- Hiv/Aids Seminar: September, 2011Documento45 páginasHiv/Aids Seminar: September, 2011Diress MollaAún no hay calificaciones
- Kimutai N Gideon Dennis Mutiso Moderator DR Songok 07 FEB 2011Documento56 páginasKimutai N Gideon Dennis Mutiso Moderator DR Songok 07 FEB 2011drgiddie7640Aún no hay calificaciones
- Patho Case 1Documento12 páginasPatho Case 1Venz Timothy Wesley LandichoAún no hay calificaciones
- Cell DifferentiationDocumento13 páginasCell DifferentiationThembi S'khandzisaAún no hay calificaciones
- HivDocumento29 páginasHivSUTHAN100% (2)
- Herpes Viruses: Viruses Causing Latent InfectionsDocumento96 páginasHerpes Viruses: Viruses Causing Latent InfectionsSolustAún no hay calificaciones
- Acquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysoreDocumento41 páginasAcquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysorerathanAún no hay calificaciones
- Viral DiagnosisDocumento37 páginasViral Diagnosissalamshakir56Aún no hay calificaciones
- Case 17 HIV-1Documento19 páginasCase 17 HIV-1ngAún no hay calificaciones
- Retrovirus: Medical Virology Dr. Saif AL-MayahDocumento11 páginasRetrovirus: Medical Virology Dr. Saif AL-MayahAtheer AlabdyAún no hay calificaciones
- ACFrOgAAdSYVz RGOOvb8Bgc gS8PfPl0WBUqI4cNvZ1Ef69iet9X10NeWzKnZYt9Z5XD vDdZSve0 O2y4GDx3XwK6KlXRf2MbWBgXnMIOGd4tEwD9UQ6 - Vhzow1NcDocumento9 páginasACFrOgAAdSYVz RGOOvb8Bgc gS8PfPl0WBUqI4cNvZ1Ef69iet9X10NeWzKnZYt9Z5XD vDdZSve0 O2y4GDx3XwK6KlXRf2MbWBgXnMIOGd4tEwD9UQ6 - Vhzow1NcAlessandro ValdezAún no hay calificaciones
- Jem 194101395Documento12 páginasJem 194101395Hamza WELGOAún no hay calificaciones
- Fusion Inhibitor and Immunomodulator AbDocumento18 páginasFusion Inhibitor and Immunomodulator AbMutiaraa Sarii DewiiAún no hay calificaciones
- Human Cytomegalovirus and Kidney Transplantation: A Clinician's UpdateDocumento9 páginasHuman Cytomegalovirus and Kidney Transplantation: A Clinician's UpdateFlorinda CarranzaAún no hay calificaciones
- Acquired Immune Deficiency Syndrome or Acquired Immunodeficiency SyndromeDocumento37 páginasAcquired Immune Deficiency Syndrome or Acquired Immunodeficiency SyndromeSumon ChowdhuryAún no hay calificaciones
- Current Perioperative Management of The Patient With Hiv A B, H M, C R, A G, A K e A.M. FDocumento12 páginasCurrent Perioperative Management of The Patient With Hiv A B, H M, C R, A G, A K e A.M. FPrashant SinghAún no hay calificaciones
- FinalDocumento42 páginasFinalVizhiAún no hay calificaciones
- HIV DISEASE - Physiotherapy ClassDocumento32 páginasHIV DISEASE - Physiotherapy ClassPraveen RajAún no hay calificaciones
- Human Immunodeficiency VirusDocumento24 páginasHuman Immunodeficiency VirusMalueth AnguiAún no hay calificaciones
- 819 FullDocumento5 páginas819 FullMinerva StanciuAún no hay calificaciones
- Comparison of Whole Blood and PBMC Assays ForDocumento5 páginasComparison of Whole Blood and PBMC Assays ForFani LonelygirlAún no hay calificaciones
- Nomenclature of Virus ProteinsDocumento11 páginasNomenclature of Virus ProteinslkokodkodAún no hay calificaciones
- HIV Life Cycle: Scott M. Hammer, M.DDocumento7 páginasHIV Life Cycle: Scott M. Hammer, M.DMohammad SalemyAún no hay calificaciones
- Cytomegalovirus InfectionDocumento18 páginasCytomegalovirus InfectionpuaanAún no hay calificaciones
- DR - Dr.efrida Warganegara, M.Kes., SP - MKDocumento30 páginasDR - Dr.efrida Warganegara, M.Kes., SP - MKDedy SantosoAún no hay calificaciones
- Chapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Documento3 páginasChapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Ernie G. Bautista II, RN, MD100% (5)
- Changes in the co-expressions of interleukin 29 (IL-29), IFN-inducible protein 10 (IP-10) and monokine induced by IFNγ (MIG) genes in chronic hepatitis C Egyptian patients untreated and treated with DAAsDocumento8 páginasChanges in the co-expressions of interleukin 29 (IL-29), IFN-inducible protein 10 (IP-10) and monokine induced by IFNγ (MIG) genes in chronic hepatitis C Egyptian patients untreated and treated with DAAsAhmed AmerAún no hay calificaciones
- Immunology 8Documento37 páginasImmunology 8ukashazam19Aún no hay calificaciones
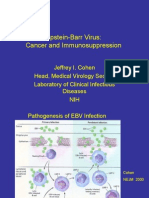
- Epstein-Barr Virus: Cancer and ImmunosuppressionDocumento31 páginasEpstein-Barr Virus: Cancer and ImmunosuppressionMoisés SantosAún no hay calificaciones
- Virology-2 MergedDocumento258 páginasVirology-2 MergedLogyn SamAún no hay calificaciones
- Human Immunodeficiency Virus, HIV: Uncategorized Leave A CommentDocumento8 páginasHuman Immunodeficiency Virus, HIV: Uncategorized Leave A Commentshrikantgautam2013Aún no hay calificaciones
- HIV&HepatitisDocumento100 páginasHIV&HepatitisRaja RuzannaAún no hay calificaciones
- AIDS Word OkokookkDocumento6 páginasAIDS Word OkokookkAlberto PiasentierAún no hay calificaciones
- Delfin, RMTDocumento34 páginasDelfin, RMTAffie SaikolAún no hay calificaciones
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureDocumento50 páginasThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianAún no hay calificaciones
- tmp320C TMPDocumento13 páginastmp320C TMPFrontiersAún no hay calificaciones
- Aid 2011 1502Documento148 páginasAid 2011 1502pasargadae_mAún no hay calificaciones
- TB MeningitisDocumento10 páginasTB Meningitisrizky ramadhanAún no hay calificaciones
- Presentation - AIDSDocumento14 páginasPresentation - AIDSPuguAún no hay calificaciones
- HEP-Adaptive Immune ResponsesDocumento7 páginasHEP-Adaptive Immune ResponsesoomculunAún no hay calificaciones
- MCD 2015 and 2016Documento6 páginasMCD 2015 and 2016Jenny LowsleyAún no hay calificaciones
- Plasma Viral Load and CD4 Lymphocytes As Prognostic Markers of HIV-1 InfectionDocumento9 páginasPlasma Viral Load and CD4 Lymphocytes As Prognostic Markers of HIV-1 InfectionStefania CristinaAún no hay calificaciones
- 2 Pa Tho Physiology of HIVDocumento8 páginas2 Pa Tho Physiology of HIVLeepin TanAún no hay calificaciones
- Chapter X HivDocumento52 páginasChapter X HivD PharmaAún no hay calificaciones
- Respiratory Disorders Case 5 HIVDocumento22 páginasRespiratory Disorders Case 5 HIVjoatasouzaAún no hay calificaciones
- Biology Ip XiiDocumento8 páginasBiology Ip XiiSugumaran MageshAún no hay calificaciones
- Clinical Tract: Module OnDocumento12 páginasClinical Tract: Module Onpschileshe9472100% (1)
- AIDS MicrobiologyDocumento42 páginasAIDS MicrobiologyRPh Krishna Chandra JagritAún no hay calificaciones
- Session 6 L Blood Borne Viruses HIV HVDocumento62 páginasSession 6 L Blood Borne Viruses HIV HVBlendma AhmedAún no hay calificaciones
- Research ArticleDocumento10 páginasResearch ArticleGregory JamesAún no hay calificaciones
- In Vivo Assessment of Antiviral Reactivity in Chronic HIV InfectionDocumento7 páginasIn Vivo Assessment of Antiviral Reactivity in Chronic HIV InfectionFrontiersAún no hay calificaciones
- HBV HCV 1Documento13 páginasHBV HCV 1Vũ Minh KhoaAún no hay calificaciones
- Immunotherapy For Sepsis - A New Approach Against An Ancient FoeDocumento3 páginasImmunotherapy For Sepsis - A New Approach Against An Ancient FoeHendy SetiawanAún no hay calificaciones
- 2 Pathophysiology of HIVDocumento8 páginas2 Pathophysiology of HIVRaga ManduaruAún no hay calificaciones
- Fast Facts: Managing immune-related Adverse Events in Oncology: Early recognition, prompt intervention, effective managementDe EverandFast Facts: Managing immune-related Adverse Events in Oncology: Early recognition, prompt intervention, effective managementAún no hay calificaciones
- Fast Facts: Managing Immune-Related Adverse Events in OncologyDe EverandFast Facts: Managing Immune-Related Adverse Events in OncologyAún no hay calificaciones
- Transfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsDe EverandTransfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsAún no hay calificaciones
- Hyperemesis GravidarumDocumento4 páginasHyperemesis GravidarumAaliyaan KhanAún no hay calificaciones
- Recombinant DNA Applications: Food IndustryDocumento2 páginasRecombinant DNA Applications: Food IndustryetayhailuAún no hay calificaciones
- Managing GMP, HSE and HTA Regulations in Multiproduct ATMP ManufacturingDocumento28 páginasManaging GMP, HSE and HTA Regulations in Multiproduct ATMP Manufacturingalnzeer omerAún no hay calificaciones
- 55 Iajps55122018 PDFDocumento4 páginas55 Iajps55122018 PDFDr.aisha KhalidAún no hay calificaciones
- DVT NotesDocumento3 páginasDVT NotesTodd EvansAún no hay calificaciones
- STS Module-Gene TherapyDocumento6 páginasSTS Module-Gene TherapyWinter SummerAún no hay calificaciones
- Preeclampsia Eclampsia and Hellp SyndromeDocumento24 páginasPreeclampsia Eclampsia and Hellp Syndromeapi-403416350100% (1)
- Revised Bioethics SyllabusDocumento7 páginasRevised Bioethics SyllabuslouradelAún no hay calificaciones
- Studiu EumastosDocumento8 páginasStudiu EumastosIoana VztAún no hay calificaciones
- 2010 - Reproduction in Domestic Ruminant Vii - LucyDocumento637 páginas2010 - Reproduction in Domestic Ruminant Vii - LucyMario MaciasAún no hay calificaciones
- AspergerDocumento7 páginasAspergerapi-508605014Aún no hay calificaciones
- WHO Meeting On Development and Evaluation of Influenza Pandemic Vaccines, Geneva, November 2-3, 2005Documento17 páginasWHO Meeting On Development and Evaluation of Influenza Pandemic Vaccines, Geneva, November 2-3, 2005jeff.aufderheide2634100% (1)
- IFA Sports Nutrition Certification Test Answer Form: Tester: Date: NameDocumento8 páginasIFA Sports Nutrition Certification Test Answer Form: Tester: Date: NameSimbarashe MabambeAún no hay calificaciones
- PBL 3 Neurotransmitter ReceptorsDocumento4 páginasPBL 3 Neurotransmitter ReceptorsJon. . .Aún no hay calificaciones
- NEET Jan 2020 PaperDocumento385 páginasNEET Jan 2020 PaperDivya RagavanAún no hay calificaciones
- Laboratory Exercise 6 1Documento10 páginasLaboratory Exercise 6 1Sofia CamamaAún no hay calificaciones
- Progress Report: Disease Team Grants by California Stem Cell AgencyDocumento44 páginasProgress Report: Disease Team Grants by California Stem Cell AgencyCalifornia Stem Cell ReportAún no hay calificaciones
- Health HistoryDocumento4 páginasHealth Historyapi-454903860Aún no hay calificaciones
- Noise Induced Hearing LossDocumento4 páginasNoise Induced Hearing LossrrrawAún no hay calificaciones
- DNA ReplicationDocumento5 páginasDNA Replicationvijayalakshmiraman100% (1)
- Differential Diagnosis of Tinea CapitisDocumento3 páginasDifferential Diagnosis of Tinea CapitisKyra KhalidAún no hay calificaciones
- Caler, 2000Documento9 páginasCaler, 2000samannosheenAún no hay calificaciones
- Disseminated Intravascular Coagulation (DIC)Documento24 páginasDisseminated Intravascular Coagulation (DIC)Atiya HajjajAún no hay calificaciones
- 1 ChromosomesDocumento9 páginas1 ChromosomesOmprakash Kumar SinghAún no hay calificaciones
- Veterinary Epidemiology (VEP-411)Documento15 páginasVeterinary Epidemiology (VEP-411)Vijay Kumar Anumolu100% (1)
- Daftar Peserta FizDocumento39 páginasDaftar Peserta FizFefin IriantiAún no hay calificaciones
- Keto Resource GuideDocumento11 páginasKeto Resource GuidejoseAún no hay calificaciones
- (Advances in Experimental Medicine and Biology 746) Tomotoshi Marumoto, Hideyuki Saya (Auth.), Ryuya Yamanaka MD, PHD (Eds.) - Glioma - Immunotherapeutic Approaches-Springer-Verlag New York (2012)Documento249 páginas(Advances in Experimental Medicine and Biology 746) Tomotoshi Marumoto, Hideyuki Saya (Auth.), Ryuya Yamanaka MD, PHD (Eds.) - Glioma - Immunotherapeutic Approaches-Springer-Verlag New York (2012)Patrick BayuAún no hay calificaciones
- Nutrition During Pregnancy and LactationDocumento240 páginasNutrition During Pregnancy and LactationDede MashaAún no hay calificaciones
- BiologyDocumento4 páginasBiologyAbanggi k sangmaAún no hay calificaciones