También podría gustarte
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
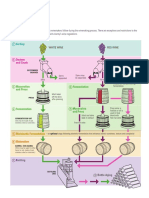
- Winemaking Booklet ProsperoDocumento44 páginasWinemaking Booklet ProsperoantonioforteseAún no hay calificaciones
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Asthma Diagnosis Monitoring and Chronic Asthma Management PDF 1837687975621Documento39 páginasAsthma Diagnosis Monitoring and Chronic Asthma Management PDF 1837687975621hisham hussainAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Medicine and SurgeryDocumento552 páginasMedicine and Surgeryhoneyjoy76100% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Adult Asthma Action PlanDocumento2 páginasAdult Asthma Action PlanantonioforteseAún no hay calificaciones
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- GINA 2019 Main Report June 2019 Wms PDFDocumento201 páginasGINA 2019 Main Report June 2019 Wms PDFAndrada PredaAún no hay calificaciones
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Asthma: Allergy Asthma and Clinical Immunology November 2011Documento10 páginasAsthma: Allergy Asthma and Clinical Immunology November 2011Sarmad AlwardiAún no hay calificaciones
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Wine GuideDocumento4 páginasWine GuidepankajkhakareAún no hay calificaciones
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Doping in Sport - ReviewDocumento5 páginasDoping in Sport - ReviewantonioforteseAún no hay calificaciones
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Stone Bee BiologyDocumento23 páginasStone Bee BiologyHRTOCAún no hay calificaciones
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- BeesInDecline PDFDocumento48 páginasBeesInDecline PDFanon_635471414Aún no hay calificaciones
- Nuclear Medicine: Science and Safety: Canadian Medical Association Journal October 1996Documento3 páginasNuclear Medicine: Science and Safety: Canadian Medical Association Journal October 1996antonioforteseAún no hay calificaciones
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- BeesInDecline PDFDocumento48 páginasBeesInDecline PDFanon_635471414Aún no hay calificaciones
- ClematisDocumento2 páginasClematisantonioforteseAún no hay calificaciones
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Genitourinary UltrasoundDocumento62 páginasGenitourinary Ultrasoundantoniofortese100% (2)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Free 12 X 8 Shed Plan - Step by Step DIYDocumento24 páginasFree 12 X 8 Shed Plan - Step by Step DIYgo2top2Aún no hay calificaciones
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Story of Honey WebDocumento11 páginasStory of Honey WebantonioforteseAún no hay calificaciones
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Backyard Gardener - Simple, Easy, and Beautiful Gardening With Vegetables, Herbs, and FlowersDocumento257 páginasThe Backyard Gardener - Simple, Easy, and Beautiful Gardening With Vegetables, Herbs, and Flowersantoniofortese100% (3)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Fuchsia CareDocumento2 páginasFuchsia CareantonioforteseAún no hay calificaciones
- Alyssum - LobulariaDocumento1 páginaAlyssum - LobulariaantonioforteseAún no hay calificaciones
- Elastography of ThyroidDocumento8 páginasElastography of ThyroidantonioforteseAún no hay calificaciones
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Growing Fuchsias in The Ground-Barbara's Way: Soil and PositionDocumento4 páginasGrowing Fuchsias in The Ground-Barbara's Way: Soil and PositionantonioforteseAún no hay calificaciones
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Achillea - YarrowDocumento1 páginaAchillea - YarrowantonioforteseAún no hay calificaciones
- Floral DiseasesDocumento3 páginasFloral DiseasesantonioforteseAún no hay calificaciones
- Acanthus Mollis - Bears BreechesDocumento1 páginaAcanthus Mollis - Bears BreechesantonioforteseAún no hay calificaciones
- DahliaDocumento2 páginasDahliaantonioforteseAún no hay calificaciones
- GAZANIADocumento1 páginaGAZANIAantonioforteseAún no hay calificaciones
- CoreopsisDocumento1 páginaCoreopsisantonioforteseAún no hay calificaciones
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- L Ily-O F-TH E-Va Lley: Featu Res ConditionsDocumento1 páginaL Ily-O F-TH E-Va Lley: Featu Res ConditionsantonioforteseAún no hay calificaciones
- Ianthus Barbatus: Sweet WilliamDocumento4 páginasIanthus Barbatus: Sweet WilliamantonioforteseAún no hay calificaciones
- Aurinia Saxat1Lis: Golden DustDocumento1 páginaAurinia Saxat1Lis: Golden DustantonioforteseAún no hay calificaciones
- SDS Safety SODIUM HYDROSULPHIDE - 2020Documento10 páginasSDS Safety SODIUM HYDROSULPHIDE - 2020KASHISH RAHEJAAún no hay calificaciones
- Unregularized Mutagenic Effects of Azo DyesDocumento13 páginasUnregularized Mutagenic Effects of Azo DyesDanish IqbalAún no hay calificaciones
- Msds Gigasept Instru AfDocumento16 páginasMsds Gigasept Instru AfDito KusumoAún no hay calificaciones
- Lecture 1 - Principles of ToxicologyDocumento119 páginasLecture 1 - Principles of ToxicologyTae-In LeeAún no hay calificaciones
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2102)
- Spider Gel - Safety AssessmentDocumento15 páginasSpider Gel - Safety AssessmentnindydputriAún no hay calificaciones
- Safety Assessment of Cucumis Sativus (Cucumber) - Derived Ingredients As Used in CosmeticsDocumento18 páginasSafety Assessment of Cucumis Sativus (Cucumber) - Derived Ingredients As Used in CosmeticsShenina KnightleyAún no hay calificaciones
- Loctite 7200 Cleaner SprayDocumento18 páginasLoctite 7200 Cleaner SprayImran MustafaAún no hay calificaciones
- Snodin 2010Documento17 páginasSnodin 2010Marvin RenteríaAún no hay calificaciones
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Desmophen 4042 BTDocumento9 páginasDesmophen 4042 BTGİZEM DEMİRAún no hay calificaciones
- 2019 Gelbke Risk Assessment For Migration of StyreneDocumento17 páginas2019 Gelbke Risk Assessment For Migration of StyreneAna Maria Lemus GranadosAún no hay calificaciones
- Chlorotoluene HPDocumento71 páginasChlorotoluene HPShailesh LahotiAún no hay calificaciones
- 5991 1876enDocumento32 páginas5991 1876enBeatriz ReyesAún no hay calificaciones
- Safety Data Sheet: Nipaguard CGDocumento18 páginasSafety Data Sheet: Nipaguard CGMaximiliano MackeviciusAún no hay calificaciones
- Biotransformation 생체전환Documento45 páginasBiotransformation 생체전환정승원Aún no hay calificaciones
- 7103LTFS (20210731)Documento15 páginas7103LTFS (20210731)anggunAún no hay calificaciones
- UNGS 2080 Assignment Essay - Zubiya PDFDocumento23 páginasUNGS 2080 Assignment Essay - Zubiya PDFZubiyaAún no hay calificaciones
- Halocur Epar Scientific Discussion - enDocumento34 páginasHalocur Epar Scientific Discussion - enSODUM DRUGSAún no hay calificaciones
- Neem by Ellen NortenDocumento100 páginasNeem by Ellen NortenMano DrabuzeliaiAún no hay calificaciones
- Acetic Anhydride MSDS - EnglishDocumento14 páginasAcetic Anhydride MSDS - EnglishMuji SyukurAún no hay calificaciones
- Prist Window Cleaner MSDSDocumento22 páginasPrist Window Cleaner MSDSSkySupplyUSAAún no hay calificaciones
- Safety Data Sheet: Section 1. IdentificationDocumento28 páginasSafety Data Sheet: Section 1. IdentificationMASAGUS MANGKU GAMAAún no hay calificaciones
- General Principles of Preclinical ScreeningDocumento15 páginasGeneral Principles of Preclinical ScreeningSumanth Kumar Reddy91% (22)
- Limites y FormulasDocumento9 páginasLimites y FormulasMercedes Carcas BadiaAún no hay calificaciones
- Aristoflex Velvet SdsDocumento14 páginasAristoflex Velvet Sdsnobel cosmeticsAún no hay calificaciones
- Loctite 480 SDSDocumento18 páginasLoctite 480 SDSwdanel2428Aún no hay calificaciones
- Genotoxic Impurities in Pharmaceutical ProductsDocumento59 páginasGenotoxic Impurities in Pharmaceutical Productsrambabukomati472100% (2)
- BIRD'S NEST EXTRACT Ver.1.1 PDFDocumento22 páginasBIRD'S NEST EXTRACT Ver.1.1 PDFjhtan84Aún no hay calificaciones
- Gigasept Instru Af ZSDB P GB enDocumento15 páginasGigasept Instru Af ZSDB P GB enKadek Ayang Cendana PrahayuAún no hay calificaciones
- Elecsys Anti-Sars-Cov-2: Safety Data SheetDocumento44 páginasElecsys Anti-Sars-Cov-2: Safety Data Sheetcargo subAún no hay calificaciones
- MSDS TerralinDocumento17 páginasMSDS Terralinfarmasi rsuassalamAún no hay calificaciones
- Summary of Mary Claire Haver's The Galveston DietDe EverandSummary of Mary Claire Haver's The Galveston DietCalificación: 5 de 5 estrellas5/5 (1)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyDe EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyCalificación: 4.5 de 5 estrellas4.5/5 (2)
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessDe EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessAún no hay calificaciones
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDe EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookCalificación: 3.5 de 5 estrellas3.5/5 (2)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)De EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Calificación: 4 de 5 estrellas4/5 (378)
- Forever Strong: A New, Science-Based Strategy for Aging WellDe EverandForever Strong: A New, Science-Based Strategy for Aging WellAún no hay calificaciones
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonDe EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonCalificación: 3.5 de 5 estrellas3.5/5 (33)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingDe EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingCalificación: 4 de 5 estrellas4/5 (3)