También podría gustarte
- Land Title Declaration FormDocumento2 páginasLand Title Declaration FormMichael Lisondra100% (1)
- Annex 1. DSWD-RLA-F001 Application FormDocumento3 páginasAnnex 1. DSWD-RLA-F001 Application FormAli NamlaAún no hay calificaciones
- If Lost, Kindly Provide Notarized Affidavit of LossDocumento3 páginasIf Lost, Kindly Provide Notarized Affidavit of LossrainrealizoAún no hay calificaciones
- Study Gap AffidavitDocumento2 páginasStudy Gap Affidavitmarge carreonAún no hay calificaciones
- Affidavit For Discharge PermitDocumento1 páginaAffidavit For Discharge Permitnorlyn esguerraAún no hay calificaciones
- Deed of Sale of MotorcycleDocumento2 páginasDeed of Sale of Motorcycleynnek0131Aún no hay calificaciones
- Deed of UndertakingDocumento2 páginasDeed of UndertakingALLAN VELEAún no hay calificaciones
- New Application Form Importer Non-Individual RMO 56-2016 - CopyDocumento1 páginaNew Application Form Importer Non-Individual RMO 56-2016 - CopyKhay-Ar PagdilaoAún no hay calificaciones
- DEED OF REAL ESTATE MORTGAGE SampleDocumento2 páginasDEED OF REAL ESTATE MORTGAGE SampleATTORNEYAún no hay calificaciones
- Ten (10) Years Roofing WarrantyDocumento2 páginasTen (10) Years Roofing WarrantyCent TorresAún no hay calificaciones
- Deed of DonationDocumento2 páginasDeed of DonationCrislene Cruz100% (1)
- Application For Securing Certificate of Compliance (Coc) : (As Indicated in DTI / SEC / CDA Registration)Documento1 páginaApplication For Securing Certificate of Compliance (Coc) : (As Indicated in DTI / SEC / CDA Registration)Francis Pascua Calumpit100% (2)
- Philippines Dues (SAR) Payment GuidelinesDocumento4 páginasPhilippines Dues (SAR) Payment GuidelinesCarlo PreciosoAún no hay calificaciones
- Complaint Form FERMIN L.Documento2 páginasComplaint Form FERMIN L.DENNIS PADOLINAAún no hay calificaciones
- NHA Form and RequirementsDocumento2 páginasNHA Form and RequirementsPrincess Manalo TafallaAún no hay calificaciones
- Revenue District Office No. 27 - Caloocan: NO. RR No. Rdo No. Bank Code Bank Name Bank Branch Bank AddressDocumento2 páginasRevenue District Office No. 27 - Caloocan: NO. RR No. Rdo No. Bank Code Bank Name Bank Branch Bank AddressCharina Marie CaduaAún no hay calificaciones
- CANDIDATE-Poll Watcher Primary-22Documento1 páginaCANDIDATE-Poll Watcher Primary-22christiandelapena50100% (1)
- Cda - Social Audit ReportDocumento58 páginasCda - Social Audit ReportJuan FrivaldoAún no hay calificaciones
- Request Letter (PCO Proposal) .2Documento1 páginaRequest Letter (PCO Proposal) .2pauldgreat2009Aún no hay calificaciones
- ReceiptDocumento2 páginasReceiptAlther Dabon100% (2)
- Undertaking Promissory NoteDocumento2 páginasUndertaking Promissory NoteCherilou Tanglao0% (1)
- Alien Employment Permit (Aep) Application FormDocumento2 páginasAlien Employment Permit (Aep) Application FormAlvin Kirby Adriatico AtienzaAún no hay calificaciones
- Contract To SellDocumento5 páginasContract To SellMarkJoven LagramaAún no hay calificaciones
- Promex Examinees PDFDocumento80 páginasPromex Examinees PDFElrich NativepigsAún no hay calificaciones
- Biodata Template PhilippinesDocumento2 páginasBiodata Template PhilippinesShannonpaz Solar100% (1)
- Reimbursement Expense Receipt Reimbursement Expense ReceiptDocumento1 páginaReimbursement Expense Receipt Reimbursement Expense ReceiptMark Calpon Lechido100% (1)
- Certificate of Appearance Form (DARLogo)Documento3 páginasCertificate of Appearance Form (DARLogo)Ricardo Saballegue100% (1)
- TCIHS STEM Entrance Exam Application FormDocumento1 páginaTCIHS STEM Entrance Exam Application FormFranz EntrataAún no hay calificaciones
- RHED Financing Application Form 1Documento2 páginasRHED Financing Application Form 1Kenneth InuiAún no hay calificaciones
- Application Form - COCOLIFE HEALTHCARDDocumento1 páginaApplication Form - COCOLIFE HEALTHCARDkimidors143Aún no hay calificaciones
- Acknowledgement ReceiptDocumento1 páginaAcknowledgement ReceiptLetski Sunga-PerezAún no hay calificaciones
- Annexes G-1 To G-5 - LTO (LPG) - RetailerDocumento7 páginasAnnexes G-1 To G-5 - LTO (LPG) - RetailerRon Realin100% (1)
- Application For Memorial Park (Final)Documento1 páginaApplication For Memorial Park (Final)Wilfredo Gabata SinoyAún no hay calificaciones
- Extrajudicial Motor - Pablo Nangit ItaraldeDocumento2 páginasExtrajudicial Motor - Pablo Nangit Itaraldejonathan basario100% (1)
- Ombudsman Letter SampleDocumento2 páginasOmbudsman Letter SampleMarjun Christopher Reyes Colipapa100% (3)
- 5 - 2019 Updates To 2009 PSIC Rules of Classification - Statistical Unitsrev05292021Documento22 páginas5 - 2019 Updates To 2009 PSIC Rules of Classification - Statistical Unitsrev05292021LGU MAHINOG MTOAún no hay calificaciones
- Sample Secretary Certificate - No Intra Corporate ActionDocumento2 páginasSample Secretary Certificate - No Intra Corporate ActionCzar Ian AgbayaniAún no hay calificaciones
- Certification: DHSUD HOACD Form No. 2021-004Documento1 páginaCertification: DHSUD HOACD Form No. 2021-004Agang Molina ColumnasAún no hay calificaciones
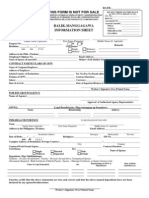
- Claimants' Statement (Coconut Farmers Group Life Insurance) : This Form Is Not For SaleDocumento2 páginasClaimants' Statement (Coconut Farmers Group Life Insurance) : This Form Is Not For SaleKhayle Naue100% (2)
- Application For Permit To Operate (New)Documento3 páginasApplication For Permit To Operate (New)RachelHechanovaAún no hay calificaciones
- Certification of Acceptance For OJTDocumento1 páginaCertification of Acceptance For OJTangelAún no hay calificaciones
- Deed of Conditional SaleDocumento2 páginasDeed of Conditional SaleLuisAdrianAmpuanAún no hay calificaciones
- Omnibus For Applying in Teacher PositionDocumento3 páginasOmnibus For Applying in Teacher PositionDenver Jane Cuyos Diacor100% (1)
- Multi-Purpose Loan Application Form (MPLAF, HQP-SLF-001, V01) EDS2Documento2 páginasMulti-Purpose Loan Application Form (MPLAF, HQP-SLF-001, V01) EDS2Edelyn Lindero Ambos100% (1)
- Acknowledgement of PaymentDocumento1 páginaAcknowledgement of PaymentMelvinson Loui Polenzo SarcaugaAún no hay calificaciones
- Cert of Site InspectionDocumento1 páginaCert of Site InspectionJohannes Gregorii LagueAún no hay calificaciones
- Annex B-2 RR 11-2018Documento1 páginaAnnex B-2 RR 11-2018Princess RegalaAún no hay calificaciones
- Asia - CEO - Awards-Nomination - Form For Mr. Chandra AnamirthamDocumento3 páginasAsia - CEO - Awards-Nomination - Form For Mr. Chandra AnamirthamalcruiseAún no hay calificaciones
- Request For Deletion of DeductionDocumento2 páginasRequest For Deletion of DeductionLeonil EstañoAún no hay calificaciones
- RDO No. 114 - Mati City, Davao OrientalDocumento694 páginasRDO No. 114 - Mati City, Davao OrientalLRM0% (1)
- Deed of SaleDocumento2 páginasDeed of SaleAlee AbdulcalimAún no hay calificaciones
- 02 BY-LAWS Amend 3Documento28 páginas02 BY-LAWS Amend 3Del Callosa100% (1)
- QuitClaim SampleDocumento1 páginaQuitClaim SampleMarcus M. Gambon100% (1)
- Certificate of Discrepancy For Scribd PDFDocumento2 páginasCertificate of Discrepancy For Scribd PDFDEAN JASPERAún no hay calificaciones
- PRLD - SRS.002-B.00 - Sworn Registration Statement (Single)Documento2 páginasPRLD - SRS.002-B.00 - Sworn Registration Statement (Single)KLASANTOS100% (1)
- Letter Request GIR PDFDocumento1 páginaLetter Request GIR PDFPearly Grace Resano100% (1)
- Deed of Absolute Sale - BlankDocumento2 páginasDeed of Absolute Sale - BlankDarwinCulaAún no hay calificaciones
- Carper Lad Form No. 70 - E Lot AlloDocumento3 páginasCarper Lad Form No. 70 - E Lot AlloLea UnderscoreAún no hay calificaciones
- Submit This Request To The Ward Clerk: Young Men Jacob Carullo 3/6/2021 Jon OcampoDocumento4 páginasSubmit This Request To The Ward Clerk: Young Men Jacob Carullo 3/6/2021 Jon OcampoJON SEBASTIAN OCAMPOAún no hay calificaciones
- Request To Deposit CheckDocumento1 páginaRequest To Deposit CheckSteven Du100% (1)
- Dale - cv1 PDFDocumento4 páginasDale - cv1 PDFDale GuerreroAún no hay calificaciones
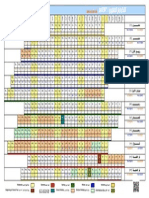
- KSA Govt Calendar 1436H (2014-2015)Documento1 páginaKSA Govt Calendar 1436H (2014-2015)Dale GuerreroAún no hay calificaciones
- Saudi Copyright Law (1424)Documento13 páginasSaudi Copyright Law (1424)Social Media Exchange AssociationAún no hay calificaciones
- Pinoy Retirement CalculatorDocumento3 páginasPinoy Retirement CalculatorDale GuerreroAún no hay calificaciones
- Final Exit Procedure From Saudi ArabiaDocumento3 páginasFinal Exit Procedure From Saudi ArabiaDale GuerreroAún no hay calificaciones
- KSA Hijri-Gregorian Calendar For 2014-1435Documento1 páginaKSA Hijri-Gregorian Calendar For 2014-1435Dale GuerreroAún no hay calificaciones
- Phil Embassy RIYADH Epassport Fillable Application Form 2 PDFDocumento0 páginasPhil Embassy RIYADH Epassport Fillable Application Form 2 PDFSurreal Beetch87% (15)
- OEC Application Eform (FOR OFWs IN SAUDI ARABIA)Documento0 páginasOEC Application Eform (FOR OFWs IN SAUDI ARABIA)Dale Guerrero100% (1)
- Kingdom of Saudi ArabiaDocumento16 páginasKingdom of Saudi Arabiam_petateAún no hay calificaciones