También podría gustarte
- Problem Behavior Interventions For Young Children With Autism: A Research SynthesisDocumento25 páginasProblem Behavior Interventions For Young Children With Autism: A Research Synthesiseebook123456Aún no hay calificaciones
- Producing Meaningful Improvements in ProblemDocumento21 páginasProducing Meaningful Improvements in ProblembrunaAún no hay calificaciones
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeDe EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriAún no hay calificaciones
- Therapist's Guide to Pediatric Affect and Behavior RegulationDe EverandTherapist's Guide to Pediatric Affect and Behavior RegulationAún no hay calificaciones
- Diagnosis and Treatment of Children With Autism Spectrum DisordersDe EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersCalificación: 5 de 5 estrellas5/5 (1)
- Treating Habit Disorders in Autism Spectrum DisorderDocumento20 páginasTreating Habit Disorders in Autism Spectrum DisorderCristian Urbano100% (1)
- Col-N Et Al-2019-Journal of Applied Behavior AnalysisDocumento18 páginasCol-N Et Al-2019-Journal of Applied Behavior Analysisnermal93100% (1)
- Dinsmoor 1995aDocumento18 páginasDinsmoor 1995ajsaccuzzoAún no hay calificaciones
- Teaching Essential Skills To Prevent Challenging Behaviour FinalDocumento22 páginasTeaching Essential Skills To Prevent Challenging Behaviour FinalAlexandra AddaAún no hay calificaciones
- Parent Training in Autism Spectrum Disorder - What's in A Name - PDFDocumento20 páginasParent Training in Autism Spectrum Disorder - What's in A Name - PDFFarbodAún no hay calificaciones
- Organizational Behavior Management in Developmental Disabilities ServicesDocumento63 páginasOrganizational Behavior Management in Developmental Disabilities ServicesMariaClaradeFreitasAún no hay calificaciones
- Cipani Instructors ManualDocumento8 páginasCipani Instructors Manualvonronge0% (3)
- BehaviorismDocumento9 páginasBehaviorismJie FranciscoAún no hay calificaciones
- WISC-V TemplateDocumento3 páginasWISC-V TemplateLindsayAún no hay calificaciones
- Measurement Techniques for Behavior AnalysisDocumento37 páginasMeasurement Techniques for Behavior AnalysisNeha AyubAún no hay calificaciones
- Evidence-Based Practice Brief: Video ModelingDocumento19 páginasEvidence-Based Practice Brief: Video ModelingIna Aulia HanifahAún no hay calificaciones
- Aba Services Handbook r2 1Documento15 páginasAba Services Handbook r2 1api-355603905Aún no hay calificaciones
- Increasing Mands PDFDocumento12 páginasIncreasing Mands PDFPamelaLiraAún no hay calificaciones
- Autism Starter KitDocumento12 páginasAutism Starter KitjoanahAún no hay calificaciones
- School-Based Interventions For Children Who Have Experienced Trauma - NASP 2010Documento72 páginasSchool-Based Interventions For Children Who Have Experienced Trauma - NASP 2010danniey66Aún no hay calificaciones
- Autism PDFDocumento41 páginasAutism PDFflower21Aún no hay calificaciones
- Data Recording: o o o o o o o o oDocumento8 páginasData Recording: o o o o o o o o oSwetha CAún no hay calificaciones
- Applied Behavior Analysis As Treatment For Autism Spectrum DisorderDocumento6 páginasApplied Behavior Analysis As Treatment For Autism Spectrum DisorderMurilo ValentimAún no hay calificaciones
- The Case of Jessica Assignment 3Documento20 páginasThe Case of Jessica Assignment 3Lara AkinpeluAún no hay calificaciones
- Functional Behavior Assesstment and Challenging Behaviors PDFDocumento45 páginasFunctional Behavior Assesstment and Challenging Behaviors PDFxs4mu3lxAún no hay calificaciones
- Training Behavior Change Agents and Parents To Implement DTTDocumento14 páginasTraining Behavior Change Agents and Parents To Implement DTTJéssica CoelhoAún no hay calificaciones
- 2 - Diagnostic Evaluation of Autism Spectrum DisordersDocumento9 páginas2 - Diagnostic Evaluation of Autism Spectrum DisordersAlice WernecAún no hay calificaciones
- Supervision OutlineDocumento9 páginasSupervision OutlineNBAún no hay calificaciones
- Evidence, Ethics, and Effectiveness of Autism InterventionsDocumento39 páginasEvidence, Ethics, and Effectiveness of Autism InterventionsVini PezzinAún no hay calificaciones
- Consequences For Problem Behavior: Rob Horner, Rhonda Nese University of OregonDocumento47 páginasConsequences For Problem Behavior: Rob Horner, Rhonda Nese University of OregonJames WangAún no hay calificaciones
- Child and AdolescentDocumento59 páginasChild and AdolescentJaezAún no hay calificaciones
- A Proposed Model For Selecting Measurement Procedures For The Assessment and Treatment of Problem Behavior PDFDocumento7 páginasA Proposed Model For Selecting Measurement Procedures For The Assessment and Treatment of Problem Behavior PDFAlina ZisuAún no hay calificaciones
- Antecedent Classroom Factors and Disruptive Behaviors of Children With Autism Spectrum DisordersDocumento18 páginasAntecedent Classroom Factors and Disruptive Behaviors of Children With Autism Spectrum DisordersJanet HeneghanAún no hay calificaciones
- The Assessment of Executive Functioning in ChildrenDocumento37 páginasThe Assessment of Executive Functioning in ChildrenYovana Estefany Lasso Caicedo100% (1)
- 5 Child and Adolescence Psychiatry-1Documento332 páginas5 Child and Adolescence Psychiatry-1abrihamAún no hay calificaciones
- A Progressive Approach to Applied Behavior Analysis: The Autism Partnership MethodDe EverandA Progressive Approach to Applied Behavior Analysis: The Autism Partnership MethodAún no hay calificaciones
- CansDocumento3 páginasCanswilliam shortAún no hay calificaciones
- Extensions of Assessment and Treatment of Food SelectivityDocumento94 páginasExtensions of Assessment and Treatment of Food SelectivityFajer AlmunayeaAún no hay calificaciones
- 10 Parenting Tricks ABADocumento13 páginas10 Parenting Tricks ABAFlora TiongAún no hay calificaciones
- Childhood Autism Rating ScaleDocumento2 páginasChildhood Autism Rating ScaleAsmaa ElarabyAún no hay calificaciones
- Iulia Mukbel - Teaching WaitDocumento10 páginasIulia Mukbel - Teaching WaitIulia Octavia MukbelAún no hay calificaciones
- Mechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeDocumento9 páginasMechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeKelly GCAún no hay calificaciones
- Main - Iwata Et Al 1982Documento18 páginasMain - Iwata Et Al 1982TimiAún no hay calificaciones
- Applied Behavior Analysis: Areas of ApplicationDocumento16 páginasApplied Behavior Analysis: Areas of ApplicationFelipe SantosAún no hay calificaciones
- The Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Documento22 páginasThe Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Ingrid DíazAún no hay calificaciones
- Rise Client Intake PackeDocumento31 páginasRise Client Intake PackeMDA therapieAún no hay calificaciones
- Presentation PDFDocumento130 páginasPresentation PDFcharraf55Aún no hay calificaciones
- Picture Exchange Communication System (PECS)Documento31 páginasPicture Exchange Communication System (PECS)Sheela Marasigan Pagkalinawan100% (1)
- Applying Structured Teaching Principles To Toilet TrainingDocumento18 páginasApplying Structured Teaching Principles To Toilet TrainingMabel FreixesAún no hay calificaciones
- Reinforcer Assessment PDFDocumento3 páginasReinforcer Assessment PDFJhan Franco Tejada FloresAún no hay calificaciones
- The Supervisory Relationship Questionnaire (SRQ)Documento3 páginasThe Supervisory Relationship Questionnaire (SRQ)kartuteAún no hay calificaciones
- NARPAA E-Class Module 8 - ABA Applied Behavior AnalysisDocumento69 páginasNARPAA E-Class Module 8 - ABA Applied Behavior Analysisnarpaa100% (1)
- Types of PsychotherapiesDocumento2 páginasTypes of PsychotherapiesJulie VictorianoAún no hay calificaciones
- Self Advocates Becoming Empowered Webinar With Autism NOW August 7 2012Documento22 páginasSelf Advocates Becoming Empowered Webinar With Autism NOW August 7 2012The Autism NOW CenterAún no hay calificaciones
- Autism Spectrum Disorder Fact SheetDocumento2 páginasAutism Spectrum Disorder Fact SheetprofjpcAún no hay calificaciones
- Parent Intake Questionnaire PDFDocumento7 páginasParent Intake Questionnaire PDFMonica TrabancoAún no hay calificaciones
- Chaining Data SheetDocumento1 páginaChaining Data SheetChangBrootAún no hay calificaciones
- Treatment For ElopementDocumento1 páginaTreatment For ElopementCarolina SilveiraAún no hay calificaciones
- ABA Autism TreatmentDocumento2 páginasABA Autism TreatmentAicee MendozaAún no hay calificaciones
- Video Modeling and Observational Learning To Teach Gaming Access To Students With ASDDocumento14 páginasVideo Modeling and Observational Learning To Teach Gaming Access To Students With ASDMaria Elisa Granchi FonsecaAún no hay calificaciones
- CR - Success StoryDocumento13 páginasCR - Success Storyapi-163017967Aún no hay calificaciones
- Kitz - Transition Plan - 2ndrevisedforschoolportfolioDocumento12 páginasKitz - Transition Plan - 2ndrevisedforschoolportfolioapi-163017967Aún no hay calificaciones
- Jkahn - BMP - RevisedforschoolportfolioDocumento9 páginasJkahn - BMP - Revisedforschoolportfolioapi-163017967Aún no hay calificaciones
- PatvelenocertificateDocumento1 páginaPatvelenocertificateapi-163017967Aún no hay calificaciones
- Ethics 5 - Vulnerable PopulationsDocumento21 páginasEthics 5 - Vulnerable Populationsapi-163017967Aún no hay calificaciones
- Jkahn - Bar - RevisedforschoolportfolioDocumento6 páginasJkahn - Bar - Revisedforschoolportfolioapi-163017967Aún no hay calificaciones
- Pats Resume - Portfolio - 2012Documento6 páginasPats Resume - Portfolio - 2012api-163017967Aún no hay calificaciones
- Assessment Plan - Case Study 1 - Veleno - Apsy693 71Documento7 páginasAssessment Plan - Case Study 1 - Veleno - Apsy693 71api-163017967Aún no hay calificaciones
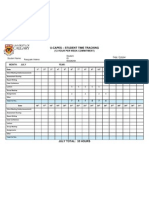
- U-Capes - Student Time Tracking: (12 Hour Per Week Commitment)Documento6 páginasU-Capes - Student Time Tracking: (12 Hour Per Week Commitment)api-163017967Aún no hay calificaciones
- KP Psyed RPT Jan 31st 2011 - RevisedforportfolioDocumento17 páginasKP Psyed RPT Jan 31st 2011 - Revisedforportfolioapi-163017967Aún no hay calificaciones
- Intervention Plan Final - Janssen Southworth Veleno - ModifiedDocumento30 páginasIntervention Plan Final - Janssen Southworth Veleno - Modifiedapi-163017967Aún no hay calificaciones
- History of Inclusive Education - Final Draft - VelenoDocumento19 páginasHistory of Inclusive Education - Final Draft - Velenoapi-163017967Aún no hay calificaciones
- Smith-Veleno - Native Tendencies Paper - Rev - ModifiedDocumento15 páginasSmith-Veleno - Native Tendencies Paper - Rev - Modifiedapi-163017967Aún no hay calificaciones
- 633-Revised1 - My Counselling TheoryassignmentDocumento26 páginas633-Revised1 - My Counselling Theoryassignmentapi-163017967Aún no hay calificaciones
- Ethics Assignment 2 - Final Version - Janssen and VelenoDocumento11 páginasEthics Assignment 2 - Final Version - Janssen and Velenoapi-163017967Aún no hay calificaciones
- Vineland-Ii Review - VelenoDocumento14 páginasVineland-Ii Review - Velenoapi-163017967100% (1)
- Parental Discipline and The Use of Aversive Procedures - VelenoDocumento23 páginasParental Discipline and The Use of Aversive Procedures - Velenoapi-163017967Aún no hay calificaciones
- Resources Assignment - VelenoDocumento26 páginasResources Assignment - Velenoapi-163017967Aún no hay calificaciones
- Veleno - Letter of Intent - Final Draft 2Documento12 páginasVeleno - Letter of Intent - Final Draft 2api-163017967Aún no hay calificaciones
- Exam Answers - Veleno - ModifiedDocumento10 páginasExam Answers - Veleno - Modifiedapi-163017967Aún no hay calificaciones
- Vineland-Ii Presentation - Monique and Pat - Final VersionDocumento22 páginasVineland-Ii Presentation - Monique and Pat - Final Versionapi-163017967Aún no hay calificaciones
- Final Copy - Review of Fasd Paper - ModifiedDocumento9 páginasFinal Copy - Review of Fasd Paper - Modifiedapi-163017967Aún no hay calificaciones
- Ed Interventions For Children With Tbi - VelenoDocumento22 páginasEd Interventions For Children With Tbi - Velenoapi-163017967Aún no hay calificaciones
- Homogeneity of Variance TutorialDocumento14 páginasHomogeneity of Variance Tutorialapi-163017967Aún no hay calificaciones
- Janssen Veleno Assignment 3Documento12 páginasJanssen Veleno Assignment 3api-87386425Aún no hay calificaciones
- Exam - Reports - Draft - Veleno - Storm - Final VersionDocumento13 páginasExam - Reports - Draft - Veleno - Storm - Final Versionapi-163017967100% (1)
- Impact of Ibi Paper - Veleno - Final Draft - ModifiedDocumento22 páginasImpact of Ibi Paper - Veleno - Final Draft - Modifiedapi-163017967Aún no hay calificaciones
- Ctopp Presentation - Second Version - ModifiedDocumento22 páginasCtopp Presentation - Second Version - Modifiedapi-163017967Aún no hay calificaciones
- LieDocumento12 páginasLieOuchaoua Ucif100% (2)
- Supplementary Material: The Genitive CaseDocumento3 páginasSupplementary Material: The Genitive CaseValentina Keilla Perez CidAún no hay calificaciones
- Applied Cryptography: Faculty Development Programme (FDP) ONDocumento2 páginasApplied Cryptography: Faculty Development Programme (FDP) ONKanakala pradeep KumarAún no hay calificaciones
- Field Study Learning Episode: On Scoring RubricDocumento4 páginasField Study Learning Episode: On Scoring Rubricaya camanggocAún no hay calificaciones
- Jasiora: Kebijakan Pengoperasian Terminal Kota Lintas Muara Bungo: Dinamika Dan PermasalahannyaDocumento13 páginasJasiora: Kebijakan Pengoperasian Terminal Kota Lintas Muara Bungo: Dinamika Dan PermasalahannyaIrfan Nurfauzan IskandarAún no hay calificaciones
- Own Two Hands Lesson PlanDocumento2 páginasOwn Two Hands Lesson Planapi-517827694Aún no hay calificaciones
- M9116 Case Study REVENUE RESIT PDFDocumento4 páginasM9116 Case Study REVENUE RESIT PDFMohammedAún no hay calificaciones
- Final Test (1-8)Documento5 páginasFinal Test (1-8)LizandRo CMAún no hay calificaciones
- Boariu Bogdan CV PDFDocumento2 páginasBoariu Bogdan CV PDFAnonymous O4ffVn8ONSAún no hay calificaciones
- FS 2 Answer SheetsDocumento80 páginasFS 2 Answer SheetsangelAún no hay calificaciones
- Abhishek Jaiswal All DocumentsDocumento20 páginasAbhishek Jaiswal All DocumentsAbhishek JaiswalAún no hay calificaciones
- Interactive Games in The Teaching-Learning Process of A Foreing LanguageDocumento20 páginasInteractive Games in The Teaching-Learning Process of A Foreing LanguageBudi UsmantoAún no hay calificaciones
- LITERATURE REVIEW Pricing StrategiesDocumento9 páginasLITERATURE REVIEW Pricing StrategiesSiraj Khan63% (8)
- The Spoken Lesson/Unspoken LessonDocumento18 páginasThe Spoken Lesson/Unspoken Lessonapi-21816946100% (1)
- Bahria Foundation College Kahuta: Islamiat Urdu Social Studies Science English Quranic Studies Computer MathsDocumento2 páginasBahria Foundation College Kahuta: Islamiat Urdu Social Studies Science English Quranic Studies Computer MathsYumna ArOojAún no hay calificaciones
- El Support Lesson Blending Words PDFDocumento9 páginasEl Support Lesson Blending Words PDFCherryMayBañolaNeonAún no hay calificaciones
- Chairman Presidential Digital Talent Program Muchemi Wambugu PDTP Report ConnectedEA2015 1-04-15Documento10 páginasChairman Presidential Digital Talent Program Muchemi Wambugu PDTP Report ConnectedEA2015 1-04-15ICT AUTHORITYAún no hay calificaciones
- Lattice Steel Towers and Steel PolesDocumento7 páginasLattice Steel Towers and Steel Polesyudha_hermawan_kinoy0% (1)
- Resume of Laminor27Documento2 páginasResume of Laminor27api-27481876Aún no hay calificaciones
- Dooley 2002 Case Study Research and Theory BuildingDocumento20 páginasDooley 2002 Case Study Research and Theory BuildingMariana VilafrancaAún no hay calificaciones
- Samarang FieldDocumento17 páginasSamarang FieldNIK NURFATIN NATASHA BINTI AHMAD DAUD BK20110288Aún no hay calificaciones
- Essay RacismDocumento4 páginasEssay Racismejqdkoaeg100% (2)
- English Lesson Plan For JSS3 First Term PDF DownloadDocumento8 páginasEnglish Lesson Plan For JSS3 First Term PDF DownloadMD Edu TechAún no hay calificaciones
- Lesson 1 Inclusive Education in Special EducationDocumento7 páginasLesson 1 Inclusive Education in Special Educationsinco lovelyn roseAún no hay calificaciones
- LINKS Supply Chain Management SimulationDocumento130 páginasLINKS Supply Chain Management Simulationrobin70929Aún no hay calificaciones
- PSY112 - 5th Exam - Problem Solving QuestionnaireDocumento2 páginasPSY112 - 5th Exam - Problem Solving QuestionnaireANDREI JONES LANGUIDOAún no hay calificaciones
- Using Story-Based Interventions To Influence People's Attitudes and Behaviour Around MoneyDocumento1 páginaUsing Story-Based Interventions To Influence People's Attitudes and Behaviour Around MoneyNkatekoChaukeAún no hay calificaciones
- 2020.relationship Between Moral Distress, WorkplaceDocumento1 página2020.relationship Between Moral Distress, WorkplaceFernandoCedroAún no hay calificaciones
- Secondary Annual Result 2023Documento1 páginaSecondary Annual Result 2023Ias motivational VideoAún no hay calificaciones
- PRBSEC-47 Internal Examination FormDocumento2 páginasPRBSEC-47 Internal Examination FormRaven OrlinoAún no hay calificaciones